I previously published an article by Smut Clyde about a certain David Geier, whom the sadistic antivaxxer and Trump-installed US Secretary of Health Robert F Kennedy Jr (RFK Jr) appointed as “senior data analyst” at the Centers for Disease Control and Prevention (CDC), to run clinical studies to prove one of the worst antivaxxer insanities – that vaccines cause autism.
“David Geier is the ideal fit to the purposes of RFK Jr. For the only reliably loyal underlings are incompetent ones who know they have no future anywhere else. ” – Smut Clyde
Because of that article, I was contacted by Kathleen Seidel who spent many years exposing the fraud and crimes committed by David Geier and his father, the original mastermind: Mark Geier, who died in March 2025. This guest post reveals that Geiers’ antivax studies were not only carbon-copies of each other, but that at least one plagiarised text from someone else’s study which eventually found NO connection between vaccine preservative thimerosal and autism. Worse: the journal editors knew, and didn’t care.
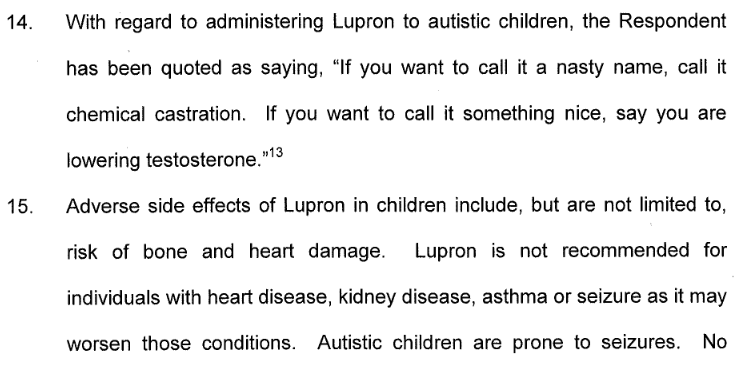
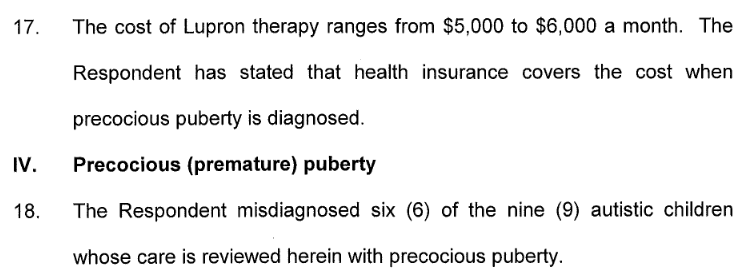
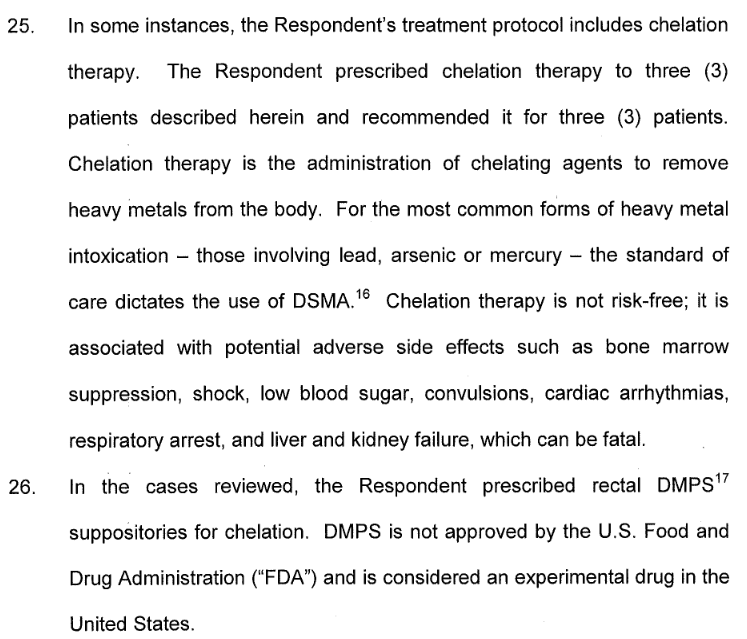
The Geiers specialised in lying, child abuse, and medical crimes. They even subjected autistic children to chemical castration treatment with the prostate cancer drug Lupron (read the Maryland Board of Physicians charges against Mark Geier, published by Elizabeth Woeckner). To call Geiers’ research on children shoddy or flawed is akin to calling a knife-stabber a shoddy surgeon who performs flawed operations.
And here are seven letters she recently submitted to the editors of five journals that published reports of the Geiers’ experiments on autistic children, and that have failed to retract them in spite of the Maryland Board of Physicians’ sanctions against both father and son:
Unfortunately, the probability of any retractions for Geiers in the foreseeable future is close to nil. Even if they cared: no journal editor or publisher would want to face the wrath of Trump, RFK Jr, and the United States government.
David and Merk Geier, photo origin unclear, provided by K Seidel
Mergers & Acquisitions by Mark and David Geier
By Kathleen Seidel
Introduction
I originally began investigating the Geiers’ work when their first peer-reviewed report of human subjects research involving autistic children was published in 2006. That led to a series of articles on my now-defunct Neurodiversity Weblog, entitled, Significant Misrepresentations: Mark Geier, David Geier, and the Evolution of the Lupron Protocol. The Maryland Board of Physicians eventually conducted an investigation that resulted in the revocation of Mark Geier’s license to practice medicine and the sanction of David Geier for practicing medicine without a license. Both disciplinary actions withstood appeal to the state’s highest court.
I stopped blogging around 2012, and stopped paying much attention to the Geiers—that is, until March 25 this year, when the Washington Postreported that David Geier had been appointed by HHS Secretary Robert F. Kennedy, Jr. to conduct a study of a possible relationship between vaccines and autism. This is exactly the sort of study that Geier père et fils had been cranking out since David joined his late father in the mass production of quasi-scientific evidence guaranteed to find an association between vaccines, mercury, autism, and whatever other substance and condition they happened to target (see reporting by New York Times and Atlantic).
Given the potential impact of such a study (especially when accorded federal imprimatur), I resumed documenting Mark Geier’s history as an expert witness in vaccine injury cases, and David Geier’s history as a dedicated parrot of his father’s litigation- and compensation-driven opinions. Their public grandstanding ultimately took the form of an antivaccinationist crusade with Mark Geier starring as the brave maverick doctor and persecuted hero, and David as his loyal sidekick.
From Liz Weil’s revealing profile in New York Magazine, we know that Mark Geier “was a quick learner,” “a bit lazy” and disinclined to hard work; that for his PhD thesis, he essentially appropriated his mentor’s work and “embellished” it some; that his primary goal was “to make a name for himself”; that he was disrespectful to both superiors and colleagues; that he felt that rules “weren’t meant for him”; and that he had little patience for the tedious work of reviewing his patients’ lab results. In spite of his scientific and medical education, he succeeded in making a name for himself not as a respected scientist, but as the sine qua non of a hired gun, willing to validate any litigant’s allegations of injury from vaccines, no matter how contrary to contemporaneous medical evidence or speculative they might be, and willing to distort and disregard inconvenient facts and evidence if they did not support his clients’ case.
Weil also notes that Mark Geier molded his son David into a replica of himself, and that David “would do anything to please his father,” including wearing matching clothing, keeping statistics of his father’s tennis matches while wearing a lab coat and stethoscope. Is it any surprise that David identified himself as a provider of “medical consulting and litigation support for personal injury attorneys” at the age of eighteen, that he would attempt to peddle “expertise” cloned from his father to the National Vaccine Injury Compensation Program (VICP), and to bill the Program for father-son trips to France and Italy, and that he would one day be sentenced by the Maryland Board of Physicians for cosplaying a doctor?
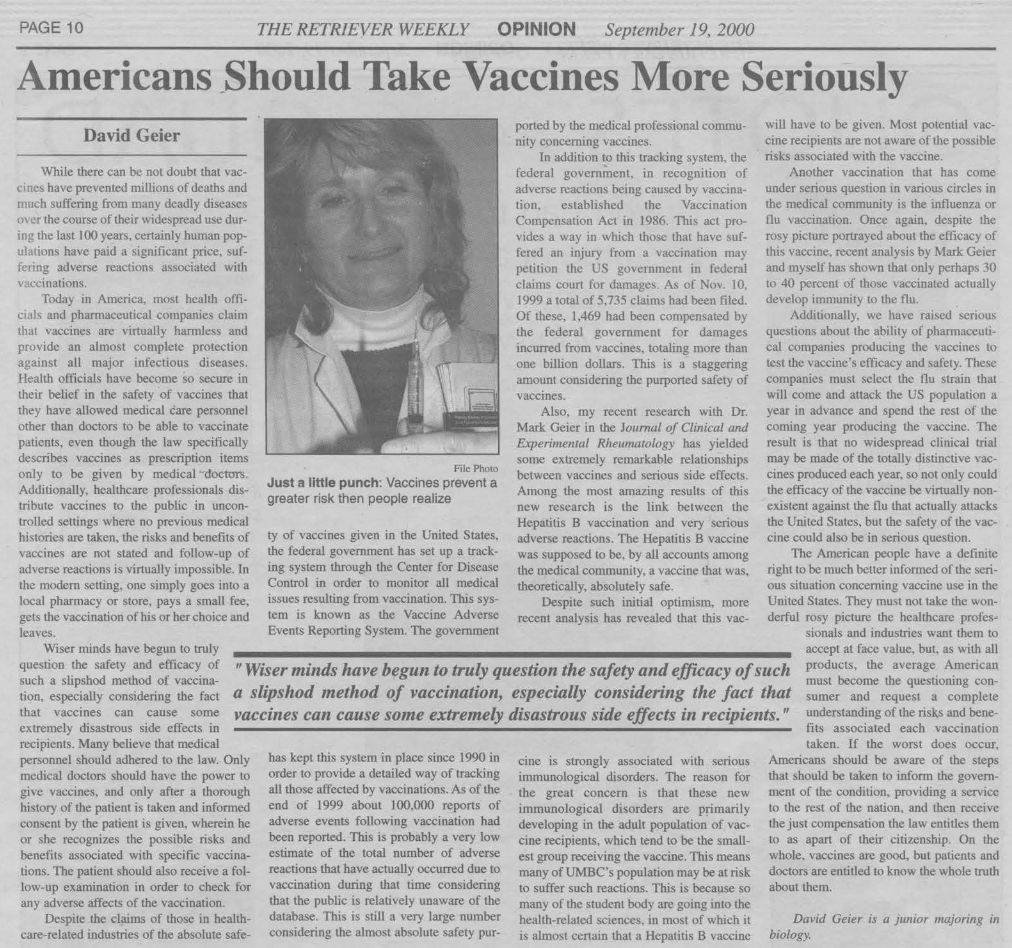
David Geier, “Elitist Protectionist Democracy America’s only Option” UMBC (2001)David Geier, “Americans _Should Take Vaccines More Seriously” UMBC (2000)
David Geier, “Manifest Destiny arid You: Why the US Should Buy Parts of Canada” UMBC (2000)David Geier, “Current Election Has Nation Returning to Combat”, UMBC (2000)
Although Mark Geier seems to have been primarily a talker with a gift for persuasion, David had a gift for writing (see above), and it is evident that his mentor in all things “sciencey” recognized how useful that talent could be to his career as an expert witness in need of peer-reviewed papers to buttress his theretofore scantily-supported opinions. Although most of Mark Geier’s scientific publications between 1978 and 1999 consisted of brief letters to editors and case reports on genetic topics, when David joined forces with his father in 2000, Mark Geier’s literary output skyrocketed, and the two became laser-focused on the topic of vaccines.
My review of the new book by Brian Deer about what became the biggest medical scandal in recent history: Andrew Wakefield’s fraudulent research on MMR vaccines and his antivax campaigning which continues even today.
The June 2000 Simpsonwood conference was a gathering of CDC officials, vaccine researchers, medical and public health professionals, some of whom were studying data from the Vaccine Safety Datalink (VSD), a collection of databases containing private medical information about millions of U.S. citizens, to ascertain possible associations between thimerosal-containing vaccines and neurological conditions. During the conference, a draft report entitled “Risk of neurological and renal impairment associated with thimerosal-containing vaccines” by Thomas Verstraeten, Robert Davis, Frank DeStefano and their colleagues (hereinafter referred to as the “2000 Verstraeten draft“) was distributed to attendees; the authors’ preliminary analyses suggested possible associations between thimerosal-containing vaccines and neurodevelopmental disorders, causing some participants to express concern about the anticipated repercussions of publishing a study that might cast doubt on the safety of childhood vaccines. Those preliminary associations did not survive subsequent analyses for confounders; the resulting study, published in the November 2003 issue of Pediatrics, concluded that
“No consistent significant associations were found between TCVs and neurodevelopmental outcomes.”
Thomas Verstraeten , Robert L. Davis , Frank DeStefano , Tracy A. Lieu , Philip H. Rhodes , Steven B. Black , Henry Shinefield , Robert T. Chen Safety of Thimerosal-Containing Vaccines: A Two-Phased Study of Computerized Health Maintenance Organization DatabasesPediatrics (2003) doi: 10.1542/peds.112.5.1039
In 2004, the 2000 Verstraeten draft and Simpsonwood conference transcript were obtained via FOIA by the organization SafeMinds, whose principals interpreted the discrepancy between preliminary analyses and the final study, and the discussion of participants’ concerns, as evidence of a massive, government- and industry-sponsored conspiracy to conceal the dangers of childhood vaccinations (cf Skeptico blog). A 2007 investigation by Senator Michael Enzi, Ranking Member of the Senate HELP Committee, concluded that their allegations were unsubstantiated. SafeMinds promptly posted the document to their website and distributed it to other organizations supporting the interests of plaintiffs in the Omnibus Autism Proceeding and other vaccine-injury litigation.
The 25th anniversary of the Simpsonwood conference provides an apt occasion for renewed examination of the extensive similarities between the 2000 Verstraeten draft and two papers by Mark and David Geier published in 2004 and 2005:
David Geier, Mark R Geier, Neurodevelopmental disorders following thimerosal-containing childhood immunizations: a follow-up analysisInternational Journal of Toxicology (2004) DOI: 10.1080/10915810490902038
David A Geier, Mark R Geier, A two-phased population epidemiological study of the safety of thimerosal-containing vaccines: a follow-up analysisMedical Science Monitor (2005) Apr;11(4):CR160-70
In “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines” (hereinafter referred to as Geier 2005), Mark and David Geier describe an evaluation of reports to the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink. The abstract summarizes their methods:
“A two phased population-based epidemiological study was undertaken. Phase one evaluated reported NDs to the Vaccine Adverse Event Reporting System (VAERS) following thimerosal-containing Diphtheria-Tetanus-acellular-Pertussis (DTaP) vaccines in comparison to thimerosal-free DTaP vaccines administered from 1997 through 2001. Phase two evaluated the automated Vaccine Safety Datalink (VSD) for cumulative exposures to mercury from TCVs at 1-, 2-, 3-, and 6-months-of-age for infants born from 1992 through 1997 and the eventual risk of developing NDs.”
The paper opens by with an announcement of a thimerosal-induced autism “epidemic,” then describes the Geiers’ study:
“The purpose of this study was to extend previous epidemiological studies, and further evaluate the relationship between thimerosal-containing childhood vaccines and neurodevelopmental disorders in a two-phase study. The first phase consisted of an epidemiological examination of the publicly available Vaccine Adverse Event Reporting System (VAERS) database for the rate of reported neurodevelopmental disorders reported following thimerosal-containing Diphtheria-Tetanus-acellular-Pertussis (DTaP) vaccines in comparison to thimerosal-free DTaP vaccines. The second phase consisted of an epidemiological examination of the Vaccine Safety Datalink (VSD) database. In examining the VSD database, an evaluation of the amount of mercury children received from thimerosal-containing vaccines at specific times in the first year of life was studied. The risk of developing neurodevelopmental disorders was determined from such exposures. The two phases of the present study were employed, so as to see if one could observe a consistent overall association between thimerosal-containing vaccines and neurodevelopmental disorders, in two entirely different databases, whilst utilizing two entirely different epidemiological methods of study.”
In their discussion of other research on autism prevalence, the Geiers state:
“There is one epidemiological study conducted in the United States that failed to report a significant association between thimerosal-containing vaccines and neurodevelopmental disorders. However, even this study by Verstaeten et al. [sic] from the CDC, initially found a significant relationship between thimerosal-containing childhood vaccines and some types of neurodevelopmental disorders, but upon further examination of a different dataset did not find a consistent effect. The lead author concluded that their study was neutral (i.e. could neither accept nor reject a causal relationship) regarding the relationship between thimerosal and neurodevelopmental disorders [29,30]. The remaining epidemiological studies that have been conducted in the United States have found a significant association between thimerosal-containing childhood vaccines and neurodevelopmental disorders [13,31-34].”
The first two citations in this passage refer to the study by Thomas Verstraeten and his then-colleagues at the U.S. Centers for Disease Control—and a 2004 Letter to the Editor of Pediatrics in which Dr. Verstraeten clarified his interpretation of his own study.
Thomas Verstraeten, Robert L Davis, Frank DeStefano, Tracy A Lieu, Philip H Rhodes, Steven B Black, Henry Shinefield, Robert T Chen; Vaccine Safety Datalink Team Safety of thimerosal-containing vaccines: a two-phased study of computerized health maintenance organization databases. Pediatrics (2003) doi: 10.1542/peds.112.5.1039
Thomas Verstraeten, Thimerosal, the Centers for Disease Control and Prevention, and GlaxoSmithKlinePediatrics (2004) doi: 10.1542/peds.113.4.932 (archived copy)
The next five citations refers to articles by the Geiers themselves, including one described as “in press”:
Geier DA, Geier MR: Neurodevelopmental disorders following thimerosal-containing childhood immunizations: a follow-up analysis.International Journal of Toxicology (2004). DOI: 10.1080/10915810490902038
Notably, the title “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines: a follow-up analysis” contains elements of the titles of the final 2003 paper by Verstraeten, et al., “Safety of thimerosal-containing vaccines: A two-phased study of computerized health maintenance organization databases,” and the Geiers’ own “Neurodevelopmental disorders following thimerosal-containing childhood immunizations: a follow-up analysis” (hereinafter referred to as Geier 2004).
Mark and David Geier submitted “Neurodevelopmental disorders following thimerosal-containing childhood immunizations” to the International Journal of Toxicology on July 16, 2004; the article was accepted on October 21, 2004, and published in their November-December 2004 issue. Four months later, the Geiers submitted “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines” to Medical Science Monitor; the article was accepted on January 19, 2005, and published in their April 2005 issue.
A paragraph-by-paragraph comparison of these two articles by the Geiers reveals many striking similarities. From the “Material and Methods” section of both articles:
The VAERS database is an epidemiological database that has been maintained by the Centers for Disease Control and Prevention (CDC) since 1990. Specific vaccine-adverse events following vaccination are required to be reported to this database as mandated by law. The VAERS Working Group of the CDC has previously reported that less than 5% of the total adverse events submitted to VAERS are reported by parents. The VAERS Working Group of the CDC and the Food and Drug Administration (FDA) analyze and publish epidemiologic studies based upon analyses of VAERS. The VAERS Working Group of the CDC published that VAERS is simple to use, flexible by design, and the data are available in a timely fashion. The authors also warn that the potential limitations in VAERS may include underreporting, erroneous reporting, frequent multiple exposures, multiple outcomes, and lack of precise denominators (Singleton et al. 1999).
The VAERS database is an epidemiological database that has been maintained by the CDC since 1990 as a surveillance tool to evaluate vaccine safety. Specific adverse events following vaccination are required to be reported to this database as mandated by law. The VAERS Working Group of the CDC has previously reported that less than 5% of the total adverse events reported to VAERS are reported by parents [7]. The VAERS Working Group of the CDC and the FDA analyze and publish epidemiologic studies based upon analyses of VAERS. They note that VAERS is simple to use, flexible by design, and the data are available in a timely fashion, but warn that the potential limitations may include systematic error due to underreporting, erroneous reporting, frequent multiple exposures, multiple outcomes and lack of precise denominators [14].
Only minor differences exist between the two passages—differences such as the position of the phrase “since 1990” in the first sentence, and the manner in which the Centers for Disease Control and the VAERS Working Group are identified.
From the “Analysis Methods” sections of both articles:
“A retrospective examination of the VAERS database (online public access version; reports entered through 28 February 2004) was undertaken using Microsoft Access. VAERS was analyzed for neurodevelopmental adverse events reported in a cohort receiving thimerosal-containing DTaP vaccines in comparison to a cohort receiving thimerosal-free DTaP vaccines (1997 through 2000), including autism, mental retardation, ataxia, speech disorders, thinking abnormalities, and personality disorders. Descriptions of these adverse events were based upon those reporting them and defined fields contained within VAERS.
The BSS of the CDC broken down by vaccine manufacturer determined the number of thimerosal-containing and thimerosal-free DTaP vaccine (1997 through 2000) doses distributed/administered. The BSS indicated that 53,579,940 thimerosal-containing DTaP vaccines and 16,915,700 thimerosal-free DTaP vaccines were distributed/administered from 1997 through 2000.
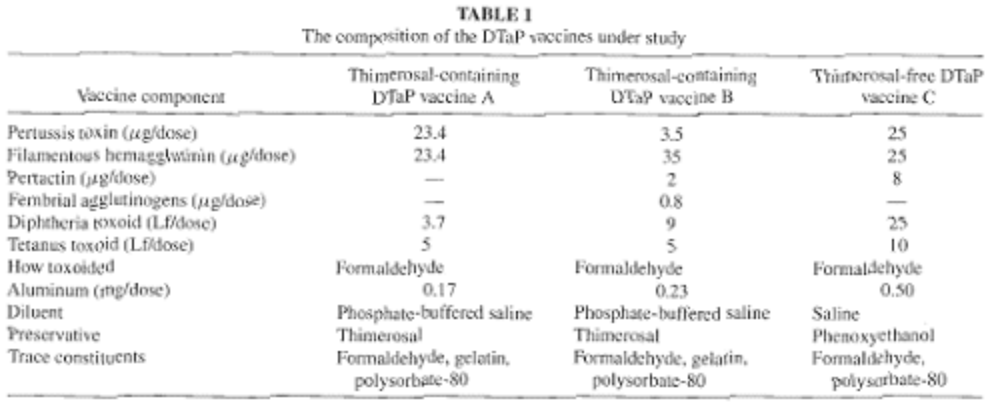
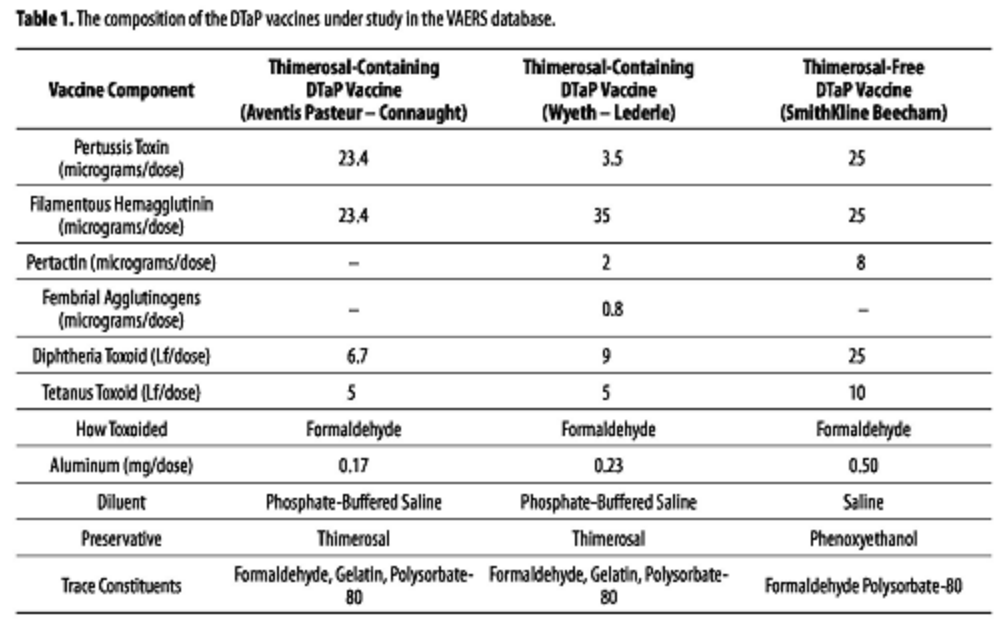
In Table 1, the composition of the DTaP vaccines analyzed are summarized.
“In the first phase of the present study, a historical examination of the VAERS database (online public access version; reports entered through 31 March 2004) was undertaken using Microsoft Access.
In this study a case-control epidemiological assessment of VAERS was undertaken by evaluating childhood neurodevelopment disorders reported following thimerosal-containing DTaP vaccines in comparison to thimerosal-free DTaP vaccines. The neurodevelopmental adverse events analyzed in VAERS included: autism (Costart Term = Autism), mental retardation (Costart Term = Mental Retard), speech disorders (Costart Term = Speech Dis), thinking abnormalities (Costart Term = Thinking Abnorm), and personality disorders (Costart Term = Person Dis). Descriptions of these adverse events were based upon those reporting them, and coded by VAERS technical staff into defined symptom fields contained in each report.
The Biological Surveillance Summaries of the CDC, as segregated by vaccine manufacturer, determined the number of thimerosal-containing and thimerosal-free DTaP vaccines (1997 through 2001) doses distributed/administered. The Biological Surveillance Summaries indicated that 59,720,009 thimerosal-containing DTaP vaccines and 29,161,630 thimerosal-free DTaP vaccines were distributed/administered from1997 through 2001.
In Table 1, the composition of the DTaP vaccines analyzed are summarized [16].
The only significant difference between the two passages lies in the final dates of the VAERS data; only four weeks’ worth of additional VAERS reports were analyzed for the 2005 article in comparison to 2004. Also, “ataxia” is included in the list of adverse events analyzed for the 2004 article. Data from both tables are identical.
From the “Controls” section of both articles:
“The distribution and geographical dispersion of the populations analyzed in VAERS were also evaluated as controls. In determining the distribution of the populations reviewed the overall mean age, total numbers of male and females reports, and male/female ratios of those reporting adverse events to VAERS were examined.
Similarly, in reviewing the geographical dispersion of the populations analyzed, the total number of adverse event reports submitted to VAERS from large representative states from the western (California), central (Illinois), and eastern (Florida) regions of the United States were examined.”
“The distribution, health status, and geographical dispersion of the data examined in VAERS were also evaluated because these factors might affect reporting of adverse events. In determining the distribution of the populations reviewed, the overall median age and total numbers of male and female reports of adverse events to VAERS were examined. In evaluating the health status of the populations reviewed, the total number of reports specifying a past medical history in VAERS was examined.
Similarly, in reviewing the geographical dispersion of the populations analyzed, one examined the total number of adverse event reports submitted to VAERS from large representative states in the western (California), central (Illinois), and eastern (Florida) regions of the US.”
The primary difference here lies in the occurrence of “health status” in the list of factors evaluated in the 2005 study. All other differences are superficial.
From the “Statistical analyses” section of both articles:
“In performing the statistical analyses employed in the present study, the premise of equality between the cohorts examined forms the basis of the null hypothesis. The statistical method involved constructing 2×2 contingency tables. We determined odds ratios (ORs), 95% OR confidence intervals (Cis) for reported adverse events, and p values from our 2×2 contingency tables.”
“The premise of equality between the groups examined forms the basis of the null hypothesis employed in the present study. Odds Ratios (OR), 95% OR Confidence Intervals (CI) for reported adverse events, and p-values were determined from 2×2 contingency tables employed in the present study.”
France is enthralled by the charm of Professor Christian Perronne. With COVID-19 almost vanquished by chloroquine magic, what about the Chronic Lyme Disease? Smut Clyde goes where even Didier Raoult refused to go.
Whereas the description of Phase I in “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines” (Geier 2005) bears a striking resemblance to “Neurodevelopmental disorders following thimerosal-containing childhood immunizations” (Geier 2004), Phase II rings other bells entirely.
Large swaths of text of the VSD portion of Geier 2005 are virtually identical to the 2000 Verstraeten draft.
“We selected a cohort of infants from the Vaccine Safety Datalink (VSD) database. VSD was created in 1991 by the National Immunization Program of the Centers for Disease Control and Prevention (CDC). The project links medical event information, vaccine history, and selected demographic information from the computerized clinical databases of four staff model health maintenance organizations (HMO)s: Group Health Cooperative of Puget Sound (GHC) in Seattle, Washington; Kaiser Permanente Northwest (NWK) in Portland, Oregon; Kaiser Permanente Medical Care Program of Northern California (NCK) in Oakland, California; and Southern California Kaiser Permanent (SCK) in Los Angeles, California. HMO members have unique HMO identification numbers that can be used to link data on their medical services within the HMO. Vaccination data are derived from computerized immunization tracking systems that are maintained by each of the HMOs. Quality control comparisons of the computerized immunization data with information recorded in paper medical records have shown high levels of agreement. For medical encounters, each of the HMOs maintains computerized databases on all hospital discharges and emergency room visits; diagnoses from outpatient clinic encounters ard available from some of the HMOs for certain years.”
“In this study, the VSD database and CDC-VSD database research materials were analyzed. VSD was created in 1991 by the NIP of the CDC. The project links medical event information, vaccine history, and selected demographic information from the computerized clinical databases of four health maintenance organizations (HMO)s: Group Health Cooperative of Puget Sound (GHC) in Seattle, Washington; Kaiser Permanente Northwest (NWK) in Portland Oregon; Kaiser Permanente Medical Care Program of Northern California (NCK) in Oakland, California; and Southern California Kaiser Permanente (SCK) in Los Angeles, California. HMO members have unique HMO identification numbers that can be used to link data on their medical services within the HMO. Vaccination data are derived from computerized immunization tracking systems, maintained by each of the HMOs. Quality control comparisons of the computerized immunization data with information recorded in paper medical records have shown high levels of agreement. For medical encounters, each of the HMOs maintains computerized databases on all hospital discharges and emergency room visits; diagnoses from outpatient clinic encounters are available from some of the HMOs for certain years [17-19]. “
The above two passages are identical, save for the first sentence, and the manner in which the National Immunization Program and the Centers for Disease Control were identified.
From the “Analysis methods” section of the 2000 Verstraeten draft, and Geier 2005:
“We have restricted our cohort to children born between 1992 and 1997 into one of the two HMOs with the most complete automated outpatient data set (GHC and NCK). For these two HMOs we have follow-up data to the end of 1998. Children in the cohort thus have a follow-up time of 1 to 7 years.
To ensure capture of all vaccination in the first year of life within the HMO, we restricted the cohort to children that were born into the HMO, continuously enrolled for the first year of life and that received at least 2 polio vaccines within the HMO y the age of 1 year. We excluded infants with ICD9 codes indicative of congenital disorders, severe perinatal disorders, recipients of HepB immunoglobulins, and gestational age less than 38 completed weeks. For this last group we performed separate analyses.”
“In the present study, as independent researchers, we analyzed data from a cohort of children born between 1992 and 1997 into one of the two HMOs with the most complete automated outpatient data sets (GHC and NCK). For these two HMOs, follow-up data to the end of 1998 was analyzed. Children in the cohort, thus, have a follow-up time of 1 to 7 years.
To ensure capture of all vaccinations in the first year of life within the HMO the cohort was restricted to children who were born into the HMO, continuously enrolled for the first year of life, and received at least 2 polio vaccines within the HMO by the age of 1 year. Infants with ICD-9 codes indicative of congenital disorders, severe perinatal disorders, recipients of hepatitis B immunoglobulins, and those who were born at gestational age of less than 38 completed weeks were excluded.”
The above two passages are strikingly similar, save for the last sentence from the 2000 Verstraeten draft, which indicates that separate analyses were conducted of data on children with specific health problems.
From the “Exposure assessment” section of the 2000 Verstraeten draft, and Geier 2005:
“We calculated the cumulative exposure to ethylmercury from individual automated vaccination records, assuming each vaccine to contain the mean dose reported by manufacturers to the FDA. We assessed this cumulative exposure at the end of the first, second, third and sixth months of life. The Thimerosal content of childhood vaccines used in the two HMOs is as follows:
“The cumulative exposure to ethylmercury from individual automated vaccination records were calculated, assuming each vaccine to contain the mean dose reported by manufacturers to the Food and Drug Administration (FDA). This cumulative exposure was assessed at the end of the first, second, third, and sixth months of life. The thimerosal content of childhood vaccines used in the two HMOs is as follows:
Hepatitis B vaccine: 25 µg (12.5 µg of mercury); Haemophilus Influenzae Type b (Hib): 50 micrograms (25 µg of mercury); Diphtheria-Tetanus-Pertussis (whole-cell or acellular): 50 micrograms (25 µg of mercury); and Polio, Mumps, Rubella, Varicella, and Pneumococcal vaccines: 0 µg of mercury.”
The above two passages are strikingly similar, save for the use of the passive voice in Geier 2005, and the Geiers’ use of the term “mercury” rather than “ethylmercury.” This modification served to obscure the difference between ethylmercury, the easily-excreted organic form of mercury found in thimerosal, and methylmercury, the inorganic form of mercury found in fish, which is far more likely than ethylmercury to accumulate harmfully in the body.
From the “Statistical analyses” section of the 2000 Verstraeten draft, and Geier 2005:
“We used a Cox proportional hazard model to compare risk of developing any of the outcomes among different levels of exposure. By stratifying on HMO, year and month of birth, we compared children born within the same month at the same HMO. We adjusted the models for gender only. By using age of the child as the time variable in the PH model we also ensured comparison of children of equal age. As endpoint we used whichever of the following occurred first: the date of first diagnosis, the date of first disenrollment from the HMO or the last day of the follow-up period, December 31, 1998. To obtain 80% power in identifying a minimal relative risk of 2, we estimated the minimal number of cases for any outcome to be 50. We subsequently evaluated the impact of increased mercury exposure on the risk of any individual outcome for which we identified at least 50 cases. Because of different coding practices between HMOs and uncertainty on the specific neurologic and renal outcomes related to mercury exposure, we also assessed the risk for the entire categories of neurologic, degenerative, neurodevelopmental and renal disorders, respectively. The category of other neurologic disorders was felt to be too heterogeneous for a similar approach. For the disorders of which we identified at least 50 cases among premature infants, we performed separate analyses for premature infants.”
“A Cox proportional hazard model was used to compare the risk of developing any of the outcomes among different levels of exposure. By stratifying on HMO, year and month of birth, children were compared that were born within the same month at the same HMO. The data were adjusted in the models for gender only. By using the age of the child as the time variable in the proportion hazard model, it was possible to ensure comparison of children of equal age. The end point used was whichever of the following occurred first: the date of first diagnosis, the date of first disenrollment from the HMO or the last day of the follow-up period, December 31, 1998. To obtain 80% power in identifying a minimal relative risk of 2, it was estimated that the minimal number of cases for any outcome to be 50. The data was evaluated to determine the impact of increased mercury exposure on the risk of any individual outcome for which at least 50 cases were identified. Because of different coding practices between HMOs, and uncertainty on the specific neurological outcomes related to mercury exposure, the data was assessed for the entire category of neurodevelopmental disorders.”
The above two passages are strikingly similar, save for the continued use of the passive voice in Geier 2005, and save for the last sentence of the 2000 Verstraeten draft, which indicates that the authors conducted separate analyses of data on children with specific health problems. The Geiers’ passive voice serves to obscure the identity of the researchers who performed the analysis.
The “Phase II Results” section of Geier 2005 contains more similarities to the 2000 Verstraeten draft:
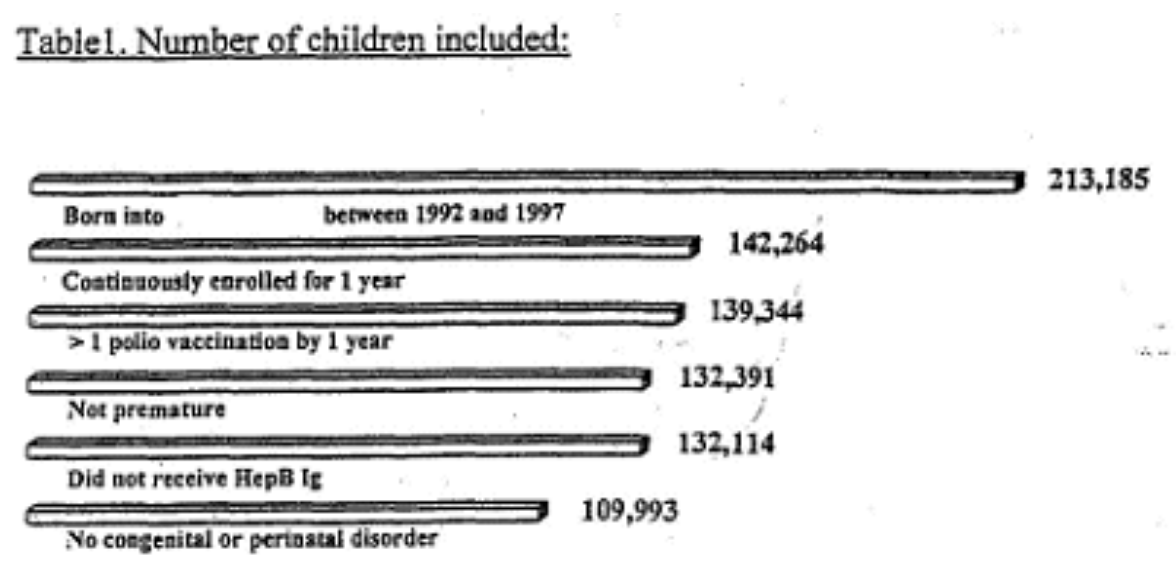
“The following table illustrates the number of children included in the cohort and the effect of the different eligibility criteria.
The final number of children thus included in our cohort was 109,993.”
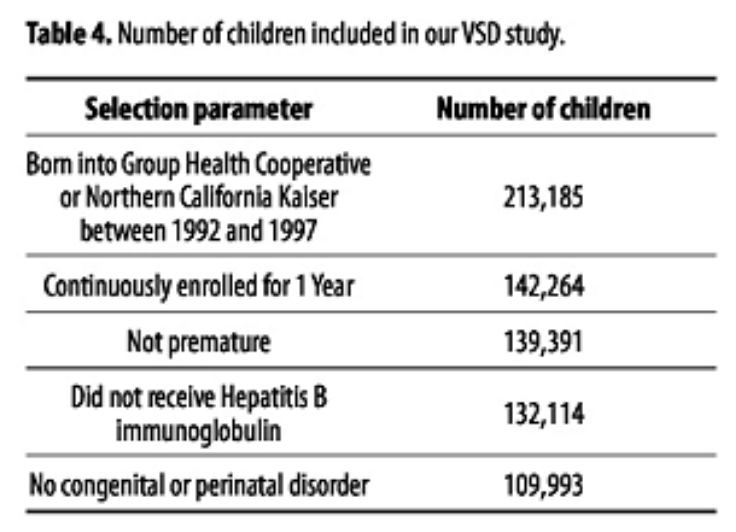
“Table 4 shows the number of children included in the cohort and the effect of the different eligibility criteria on the present assessment of the VSD database. The final number of children thus included in the cohort examined was 109,993.
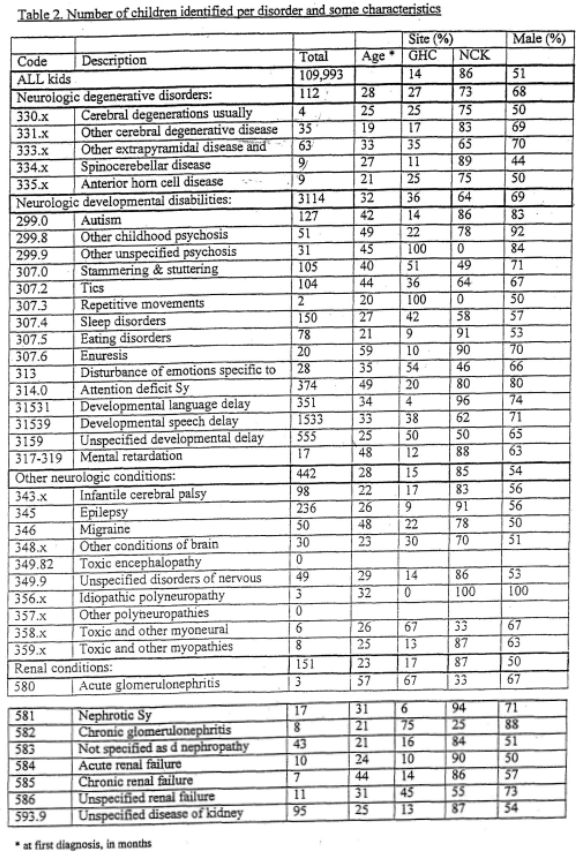
“Table 2 shows the number of cases encountered for each disorder, the mean age at first diagnosis, the distribution over the two HMOs and the percentage males among cases.
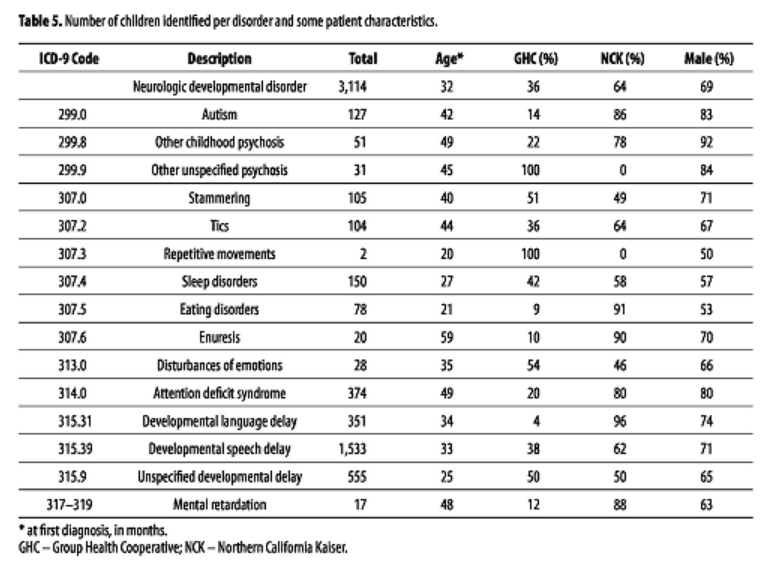
“Table 5 shows the number of cases encountered for each disorder, the mean age at first diagnosis, the distribution over the two HMOs, and the percentage males among cases.
The data in both tables and the manner of describing them are virtually identical, save for the inclusion in the 2000 Verstraeten draft of the category, “>1 polio vaccination by 1 year.”
The data in the Geier table are identical to the data contained in the “Neurologic developmental disabilities” portion of the 2000 Verstraeten draft. The manner of describing the two charts is identical.
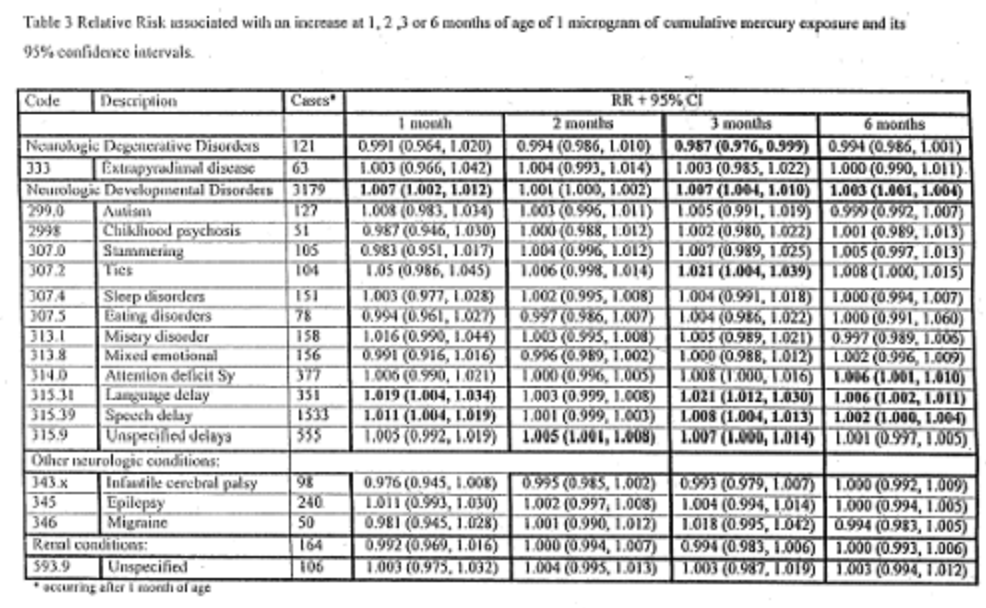
“Results for risk estimates are given first for the cumulative mercury exposure as a continuous variable assessed at 1, 2, 3, and 6 months of age. Table 3 shows the number of cases occurring any time after the point at which the exposure is assessed, the relative risk estimate, and its 95% confidence intervals, associated with an increase of 1 microgram of cumulative mercury exposure at 1, 2, 3, or 6 months of age… [S]tatistically significant results (not adjusting for multiple comparisons) are bolded.
The relative risks and confidence intervals reported in Geier 2005 are identical to those reported in Table 3 of the 2000 Verstraeten draft.
In Geier 2005, a single instance of the active voice occurs in the first section of the Phase II (VSD) “Analysis Methods” section:
“In the present study, as independent researchers, we analyzed data from a cohort of children born between 1992 and 1997 into one of the two HMOs with the most complete automated outpatient data sets (GHC and NCK).”
It is likely that this statement is false given the absence of any statement of Institutional Review Board (IRB) approval of the study. All research involving the Vaccine Safety Datalink requires approval by an IRB, since it is composed of private medical records of U.S. citizens—that is, human subjects—whose health care providers are legally required to safeguard their patients’ medical information.
Smut Clyde takes on Dr Judy Mikovits and guides you through her career, from fake Science to antivax and cancer quackery, and over to COVID-19 conspiracies, in 5 acts plus Coda.
Echoes of “Neurodevelopmental disorders following thimerosal-containing childhood immunizations” (Geier 2004) resound in the Discussion portion of “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines: a follow-up analysis” (Geier 2005).
“In further considering the results of the present study, if must be noted that none of the children we examined in this study from the VAERS database truly represent a background population that received no thimerosal. It was observed among the reports examined in the VAERS database that other vaccines containing thimerosal, such as hepatitis B vaccine, Haemophilus influenza type B (Hib) vaccine, or influenza vaccine, were concurrently administered in the birth cohorts examined. The central difference in the total amounts of mercury received from thimerosal-containing vaccines in the children examined in the VAERS database stems from the fact that some children received additional doses of mercury from thimerosal-containing DTaP vaccine in comparison to those children receiving thimerosal-free DTaP vaccine. As a result, the increased risks observed for neurodevelopmental disorders, probably represent a considerable underestimation of the true risk of additional doses of mercury from thimerosal containing vaccines.
As far as exposure from other sources that may have had significant concentrations of mercury such as Rho immune globulin, seafood, manufacturing plant emissions, dental amalgams, and/or other pharmaceuticals, although potentially significant, probably had a limited effect on the results of this study because the populations analyzed were large, and there should have been equal exposure to other sources of mercury among the populations examined. The probability that exposure to other sources of mercury were similar in the thimerosal-containing and thimerosal-free DTaP vaccine cohorts examined in the VAERS database is further supported by the fact that there were similar geographical dispersions in the populations examined.”
“In further considering the results of the present study, it must be noted that none of the children examined in this study of the VAERS database truly represent a thimerosal-free population. Within the reports, it was observed that other vaccines containing thimerosal such as hepatitis B vaccine, Hib vaccine, or influenza vaccine were concurrently administered to those receiving thimerosal-containing or thimerosal-free DTaP vaccines. The difference in the total amounts of mercury received from thimerosal-containing vaccines in the children examined in the VAERS database stems from the fact that some children received additional doses of mercury from thimerosal-containing DTaP vaccine in comparison to those children receiving thimerosal-free DTaP vaccine. As a result, the increased risks observed for neurodevelopmental disorders, probably, represent a considerable underestimate of the true risk of additional doses of thimerosal from vaccines.
Other sources of mercury such as anti-Rhoimmune globulin, seafood, manufacturing plant emissions, dental amalgams, and other pharmaceuticals, while potentially significant, probably had a limited effect on the VAERS results of this study because the populations analyzed were large, and there should have been equal exposure to other sources of mercury among the populations examined. The probability that exposure to other sources of mercury were similar, among those receiving thimerosal-containing or thimerosal-free DTaP vaccines, is further supported by the fact that there were similar geographical dispersions and health statuses in both groups.”
Mark and David Geier then describe limitations of their study in a manner and order virtually identical to the 2000 Verstraeten draft.
“Limitations: Some misclassification errors may have occurred in the assessment of the inclusion/exclusion criteria: some HepB Ig administrations may be missed, some premature children may not be classified as such. In case of a true effect of thimerosal, this error is likely to cause a bias towards the null hypothesis.
Some misclassification error may have occurred in the exposure assessment: some vaccinations, particularly the neonatal HepB dose may not have been reported. We estimated that approximately 4 and 18% of these are missed at NCK and GHC respectively. In case of a true effect of thimerosal, this error is likely to cause a bias towards the null hypothesis.
We were not able to differentiate, using the available automated data, between single dose thimerosal free Hib vaccines and multi-dose thimerosal containing Hib vaccines. The analyses were done assuming all vaccines to come from multi-dose vials. An analysis assuming all Hib vaccines to come from single dose vials did not substantially alter the results. An ongoing FDA effort to resolve this question based upon the lot numbers has revealed that about 1% of the Hib vaccines may be Thimerosal free. In case of a true effect of thimerosal, this error would cause a bias towards the null hypothesis.”
“In considering the results from the VSD database, there may have been some limitations. Some misclassification errors may have occurred in the assessment of the inclusion/exclusion criteria: some hepatitis B immunoglobulin administrations may have been missed and some premature children may not have been classified as such.
Some misclassifications error may have also occurred in the exposure assessment: some vaccinations, particularly the neonatal hepatitis B vaccine dose, may not have been reported.
It is not always possible to differentiate, using the available automated data, between single dose thimerosal-free Hib vaccines and multi-dose thimerosal-containing Hib vaccines. The analyses were done assuming all vaccines to come from multi-dose vials. An analysis assuming all Hib vaccines had come from single dose-vials did not substantially alter the results. It is likely that in the case of a true effect of thimerosal, all of these sources of potential errors were likely to bias towards the null hypothesis.”
“A lack of specificity in the ICD9 codes for congenital or perinatal disorders may have caused exclusion of children that were not at higher risk for developmental disorders and/or lower risk for vaccination. This error is likely to have decreased the power. Including all children regardless of these disorders results in moderate changes in results towards the null.
Some misclassification error may have occurred in the outcome assessment: we used ICD9 codes from automated data that lack specificity for certain disorders and are prone to errors by the person (often administrative) coding and at data entry level. This error is likely to cause an error in the findings for some specific ICD9 codes that may not have an obvious clinical correlate such as 315.39 (other developmental speech or language disorder) or 315.9 (unspecified delay in development). There is not reason to think that this error would occur differentially among the exposure categories and it is therefore unlikely to affect the estimates.”
“Some misclassification errors may have occurred in the outcome assessment in the VSD database as ICD-9 codes, that lack specificity for certain disorders and are prone to errors by the person (often administrative) coding and at data entry level, were used from automated data. Such misclassification is likely to cause an error in the findings for some specific ICD-9 codes that may not have an obvious clinical correlate such as ICD-9 code 315.30 (other developmental speech or language disorder) or ICD-9 code 315.9 (unspecified delay in development). There is no reason to think that this error would occur differentially among the exposure categories, and it is, therefore, unlikely to affect the results of our assessment of the VSD database.”
“We had no information on potential predisposing factors, such as maternal smoking, lead exposure or fish consumption. It is not clear, however, how these factors would be related to the exposure measure and are felt to be unlikely to cause any bias.”
“Additionally, no information was available on potential predisposing factors, such as maternal smoking, lead exposure or fish consumption in this assessment of the VSD database. However, it is not clear how these factors would be related to the exposure measured and are felt to be unlikely to cause any bias, as they would be expected to occur equally in all exposure groups examined.”
“We have limited our analyses to a list of potential outcomes based on prior knowledge of adverse conditions found in infants exposed to high doses of methylmercury. We cannot rule out other disorders potentially related to exposure to ethylmercury.”
“It is also important to realize that in the present assessment of the VSD database, analyses were limited to a list of potential outcomes based upon results gleaned from the VAERS database assessment. Other disorders potentially related to exposure to ethylmercury cannot be ruled-out.”
“We were able to evaluate only relatively severe conditions that come to medical attention, and not possibly more subtle effects. Such an evaluation would require neuropsychological testing.”
“Only relatively severe conditions that come to medical attention in this assessment of the VSD database could be evaluated in the present study, and more subtle effects that would require neuropsychological testing could not be studied.”
“These people are anti-Cassandras… they are optimistic and always wrong, receiving endless interviews about the censorship of their views, while their confident opinionation is always taken respectively by other Public Intellectuals because they are Serious People.” – Smut Clyde
Mark and David Geier eventually refer to studies contradicting their own conclusions, and to studies that ostensibly support them—many of their own, or by researchers recommended by SafeMinds, whose founding goal was “to encourage and support efforts to conduct medical research that provides credible findings to support that the mercury/autism hypothesis is true”—in other words, to support research that promises to validate the founders’ pre-existing conclusions about autism causation, and advance the political and legal agenda of vaccine-injury plaintiffs.
“A recent clinical study by Bradstreet et al. (2003) has evaluated the concentration of heavy metals in the urine among children with autistic spectrum disorders in comparison to a neurotypical control population based upon excretion following a 3-day treatment with meso 2,3-dimercaptosuccinic acid (DMSA). The authors observed that there was approximately six-times significantly greater urinary mercury concentrations among vaccinated cases matched to vaccinated neurotypical controls, whereas children with autistic spectrum disorders had similar urinary cadmium and lead concentrations in comparison to controls. Similar urinary mercury concentrations were observed among matched vaccinated and unvaccinated neurotypical children following DMSA treatment.
Similarly, Holmes et al. (2003) have evaluated body-burdens of mercury by examining postnatal mercury elimination in first baby haircut samples from 94 children diagnosed with autism in comparison to 45 age- and gender-matched controls.
…Together, these clinical observations suggest that autistic children have significantly higher body-burdens of mercury than neurotypical children following exposure to mercury.”
“The biochemical and genomic basis for the increased body-burden of mercury in autistic children have been identified. James et al. (in press a) have evaluated the methionine-cycle and transsulfuration metabolites in autistic children in comparison age- and sex-matched control children. It was determined that there were significant decreased in the plasma concentration of cysteine (19% reduction) and glutathione (46% reduction), both are crucial for mercury excretion, in autistic children in comparison to control children. Additionally, consistent with the DMSA treatment and first baby haircut study results, it was determined that autistic children had significantly increased oxidative stress (3-fold decrease in glutathione/oxidized glutathione redox ratio) in comparison to control children. Boris et al. (in press) have identified specific genomic polymorphisms for enzymes in the methionine cycle and transsulfuration pathways in autistic children that would account for the distinct transsulfuration metabolite profiles observed by James et al. in autistic children.
A decreased ability to excrete mercury is troubling because thimerosal has been reported by a researcher from the Food and Drug Administration (FDA) to cross the blood-brain and placental barriers, and result in appreciable mercury content in tissues, including the brain (Slikker 2000). In addition, it has recently been shown there was an approximate 28 day half-life of mercury in the brains of young primates injected with thimerosal solutions that had similar concentrations to thimerosal-containing childhood vaccines (Institute of Medicine 2004).”
“A recent clinical study by Bradstreet et al. evaluated the concentration of heavy metals in the urine among a population of children with autistic spectrum disorders in comparison to a neurotypical control population [35]. Based on excretion following an identical three-day oral provocation with meso2,3-dimercaptosuccinic acid (DMSA), it was observed that there were approximately 6-times significantly greater urinary mercury concentrations among vaccinated cases matched to vaccinated neurotyptical controls, whereas children with autistic spectrum disorders had similar urinary cadmium and lead concentrations in comparison to neurotypical controls. Similar urinary mercury concentrations were observed among matched vaccinated neurotypical children and unvaccinated neurotypical children following DMSA treatment.
Similarly, Holmes et al. have examined the ability to excrete mercury by examining mercury levels in the first baby haircuts of autistic children in comparison to non-autistic control children [36].
…Together, these clinical observations suggest that autistic children have significantly higher body-burdens of mercury than neurotypical children following exposure to mercury.”
“The biochemical and genomic basis for the increased body-burden of mercury in autistic children have been identified. James et al. have evaluated the methionine cycle and transsulfuration metabolites in autistic children in comparison to age and sex-matched control children [37,38]. It was determined that there were significant decreases in the plasma concentration of cysteine (19% reduction) and glutathione (46% reduction), both of which are crucial for mercury excretion, in autistic children in comparison to control children. Additionally, consistent with the DMSA treatment and first baby haircut study results, it was determined that autistic children had significantly increased oxidative stress (3-fold decrease in glutathione/oxidized glutathione redox ratio) in comparison to control children. Researchers have also identified specific genomic polymorphisms for enzymes in the methionine cycle and transsulfuration pathways in autistic children that would help to account for the distinct transsulfuration metabolite profiles observed by James et al. in autistic children [37,39].
The inability to properly eliminate mercury is particularly troubling since it was shown by Gasset et al. that administration of thimerosal to animals resulted in a substantial concentration of mercury present in blood and tissues (including the brain) of the treated animals and their offspring [40]. The authors concluded that thimerosal crosses the blood-brain barrier and placental barriers. Similarly, Slikker from the FDA has confirmed that thimerosal crosses the blood-brain barrier and placental barriers and results in appreciable mercury content in tissues including the brain [41]. Sager has recently reported the half-life of mercury in the brain of infant primates was approximately 28 days following administration of solutions containing vaccine comparable concentrations of thimerosal [42].”
“Leong, Syed, and Lorscheider (2001) recently examined neurite outgrowth following exposure to the same concentrations of mercury, aluminum, lead, cadmium, and manganese, demonstrating that nanomolar (nM) concentrations of mercury markedly disrupted membrane structure and linear growth rates of imaged neurites in 77% of all nerve growth cones. It was observed that the tubulin/microtubule structure disintegrated following mercury exposure. In contrast, exposure to other metal ions did not affect growth cone morphology, or their motility rate. The authors reported in the presence of mercury, neuronal somata failed to sprout, whereas the other metals examined did not affect growth patterns of the neurons examined, providing visual and biochemical evidence that strongly implicated mercury as an etiological factor in neurodegeneration. Similar results have been observed in tissue culture systems with thimerosal (Brunner, Albertini, and Wurgler 1991; Parry 1993; Wallin and Hartely-Asp 1993).”
“Leong et al. recently examined neurite outgrowth following exposure to the same concentrations of mercury, aluminum, lead, cadmium, and manganese. The authors demonstrated that nanomolar (nM) concentrations of mercury markedly disrupted membrane structure and linear growth rates of imaged neurites in 77% of all nerve growth cones, whereas the other metals examined did not affect growth patterns of the neurons examined. The authors concluded that their study provides visual and biochemical evidence strongly implicating mercury as a potent factor in neurodegeneration [44]. Similar results have been observed in tissue culture systems with thimerosal [45-47].”
“In addition, James et al. (in press b) have reported that the neurotoxicity of thimerosal is associated with depletion of glutathione. The ethylmercury in thimerosal binds to cysteine thiol (-SH) groups on intracellular proteins and inactivates their function. The cysteine-SH group of glutathione, binds mercury and protects essential proteins from functional inactivation. Glutathione is the major mechanism of mercury excretion, and individuals with genetic deficiencies in glutathione synthesis will be less able to excrete mercury and will be more sensitive to its adverse effects.”
“In addition, it has been reported that the neurotoxicity of thimerosal is associated with depletion of glutathione. The ethylmercury in thimerosal binds to cysteine thiol (-SH) groups on intracellular proteins and inactivates their function. The cysteine-SH group of glutathione binds mercury and protects essential proteins from functional inactivation. Glutathione is the major mechanism of mercury excretion, and individuals with genetic deficiencies in glutathione synthesis will be less able to excrete mercury and will be more sensitive to its adverse effects [37-48].”
“Waly et al. have reported that methylation events play a critical role in the ability of growth factors to promote normal development. The authors found that insulin-like growth factor-1 (IGF-1)- and dopamine-stimulated methionine synthase (MS) activity and folate-dependent methylation of phospholipids in SH-SY5Y human neuroblastoma cells, occurred via a phosphoinositol (PI) 3-kinase- and mitogen-activated protein (MAP) kinase-dependent mechanism. The stimulation of this pathway increase3d DNA methylation, whereas its inhibition increased methylation-sensitive gene expression. Thimerosal inhibited both IGF-1 and dopamine-stimulated methylation, with an IC50 of 1 nM, and eliminated MS activity. The authors concluded that the discovery of the PI3-kinase/MAP-kinase/MS pathway, and its potent inhibition by thimerosal, a vaccine component, provides a molecular explanation for how increased use of vaccines could promote an increase in the incidence of autism and Attention-Deficit-Hyperactivity-Disorder (ADHD). In addition, Deth and Waly (2004) have reported that folate-dependent, phospholipid methylation in the lymphoblasts of autistic children were in a dose-response manner, significantly more sensitive to thimerosal exposure than in unaffected siblings [50].”
“Waly et al. have reported that methylation events play a critical role in the ability of growth factors to promote normal development [49]. The authors found that insulin-like growth factor-1 (IGF-1) and dopamine-stimulated methionine synthase (MS) activity and folate-dependent methylation of phospholipids in SH-SY5Y human neuroblastoma cells, occurred via a PI3-kinaseand MAP-kinase-dependent mechanism. Thimerosal inhibited both IGF-1anddopamine-stimulated methylation with an IC(50) of 1 nM and eliminated MS activity. The authors concluded that the discovery of the PI3-kinase/MAP-kinase/MS pathway, and its potent inhibition by thimerosal, a vaccine component, provides a molecular explanation for how increased use of vaccines could promote an increase in the incidence of autism and Attention-Deficit-Hyperactivity-Disorder (ADHD). In addition, Deth and Waly have reported that folate-dependent, phospholipid methylation in the lymphoblasts of autistic children were, in a dose-response manner, significantly more sensitive to thimerosal exposure than in unaffected siblings [50].”
Yehuda Shoenfield is either a genius or a quack of autoimmunity research, depending on which side you stand in the antivax debate. He is also apparently a plagiarist, even Wikipedia is not safe. And this is why he is now a Member of Israel Academy of Sciences.
In both Geier 2004 and Geier 2005, the authors acknowledge their most significant source of bias: their professional involvement in vaccine-injury litigation.
“Potential conflict of interest: David Geier has been a consultant in cases involving vaccines before the no-fault National Vaccine Injury Compensation Program (NVICP) and in civil litigation. Dr. Mark Geier has been an expert witness and consultant in cases in involving vaccines before the no-fault NVICP and in civil litigation.”
“Potential conflict of interest: Dr. Mark Geier has been an expert witness and consultant in cases in involving vaccines before the no-fault National Vaccine Injury Compensation Program (NVICP) and in civil litigation. David Geier has been a consultant in cases involving vaccines before the no-fault NVICP and in civil litigation.”
Misleadingly, that involvement was expressed in the past tense; at the time the article was published, both father and son had an active contract to provide services to petitioners in the Omnibus Autism Proceeding.
Whose Words Are They, Anyway?
As mentioned above, Mark and David Geier submitted “Neurodevelopmental disorders following thimerosal-containing childhood immunizations” (Geier 2004) to the International Journal of Toxicology on July 16, 2004; the article was accepted for publication on October 21, 2004. They submitted “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines: a follow-up analysis” (Geier 2005) to Medical Science Monitor on November 17, 2004—four months after submitting their previous article to the International Journal of Toxicology, and four weeks after its acceptance for publication.
The International Journal of Toxicology’s Instructions for Authors state:
“All accepted manuscripts, artwork, and photographs become the property of the American College of Toxicology.”
Medical Science Monitor’s Instructions for Authors state:
“Medical Science Monitor is an international, peer-reviewed scientific journal that publish original articles in experimental and clinical medicine and related disciplines such as molecular biology, biochemistry, genetics, biophysics, bio- and medical technology… It is understood that all authors listed on a manuscript have agreed to its submission… Materials taken from other sources must be accompanied by a written statement from both author and publisher giving permission to the Journal for reproduction. Obtain permission in writing from at least one author of papers still in press, unpublished data, and personal communications.
Editorial Board of Medical Science Monitor takes under consideration for publication original articles in experimental and clinical medicine and related disciplines with the understanding that neither the manuscript nor any part of its essential substance, tables or figures have been published previously in print form or electronically and are not under consideration by any other publication or electronic medium. Copies of any closely related manuscripts should be submitted to the Editor along with the manuscript that is to be considered by the Journal. The Journal discourages the submission of more than one article dealing with related aspects of the same study.”
In spite of the extensive similarities between Geier 2004, the 2000 Verstraeten draft, and Geier 2005, and in spite of the copyright restrictions that applied to Geier 2004 after its acceptance for publication, Geier 2005 was published by Medical Science Monitor in the Spring of 2005, represented as solely and originally authored by Mark and David Geier. Although the byline notes indicate that both authors contributed to study design, data collection, statistical analysis, data interpretation, manuscript preparation, and literature search, there is no indication that their “data collection” might have entailed collecting data from another research group’s study, or that their “manuscript preparation” might have entailed merging that study with an article they had previously written, making little more than superficial textual modifications and references to a few newly-published journal articles by their colleagues.
Aristidis Tsatsakis, Konstantinos Poulas, Ronald Kostoff, Michael Aschner, Demetrios Spandidos, Konstantinos Farsalinos: you will need a disinfecting shower once you read their papers.
One notable passage appeared in “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines” that did not appear in the Geier’s previous papers:
“We wish to thank Lisa Sykes for her kind efforts in helping us to review and edit our manuscript.”
Rev. Lisa Sykes is a now-retired Methodist minister, fervent admirer of Geiers (she wrote the March 2025 obituary for Mark Geier) , co-founder with the Geiers of the Coalition for Mercury-Free Drugs (CoMED), unsuccessful plaintiff in Sykes v. Glaxo SmithKline (aka Sykes v. Bayer) (a federal lawsuit in which this author was unsuccessfully subpoenaed), co-author with David Geier of the autohagiography Sacred Spark, and a true believer in the idea that her autistic son was poisoned by mercury in his vaccines, in the RhoGAM shot she received while pregnant, and in environmental emissions by Dominion Electric.
On November 5, 2004, Rev. Sykes submitted to the FDA Division of Dockets Management a comment to FDA Docket #2004P-0349—a Citizens’ Petition which she had originally filed on behalf of herself and four other CoMED representatives, demanding the removal of thimerosal from vaccines. In her comment, Rev. Sykes made numerous allegations of criminal wrongdoing and referred to the 2000 Verstraeten draft.
“The CDC, Food and Drug Administration (FDA), and pharmaceutical companies colluded at the Simpsonwood Retreat Center in Norcross Georgia on June 7 and 8, 2000. At this closed meeting, a CDC study authored by Thomas Verstraeten was discussed. The scientists, CDC, FDA and pharmaceutical officials acknowledged the statistical correlation between mercury exposure through pediatric vaccines and neurological disorders in children including autism, ADHD, stuttering, tics and speech and language delays. This version of the Verstraeten study was never released to the public and could only be accessed through the Freedom of Information Act (FOIA). Evidence of their collusion is recorded in the Simpsonwood Transcripts, also accessed through FOIA.”
It is evident from the Geiers’ acknowledgment that the conspiracy-mongering minister was familiar with the contents of “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines.” It is evident from her comment to the FDA that by November 5, 2004, she was also familiar with the contents of the 2000 Verstraeten draft, which had been posted to the SafeMinds and NoMercury websites shortly before October 11, 2004.
In her comment to FDA, Rev. Sykes claimed the moral high ground, urging federal regulators to “study the science that has already been worked out” by researchers sympathetic to the cause of vaccine-injury plaintiffs:
“As one trained in ethics, and specifically in medical ethics, I challenge you to resist institutional inertia, and rapidly study the science that has already been worked out by Dr. Megson, Dr. Wakefield, Dr. McGinnis, Dr. Holmes and Dr. Cave.”
It is evident that Rev. Sykes’ “specific training in medical ethics” did not make her particularly alert to or concerned about either the similarities between the 2000 Verstraeten draft and the article she helped to edit, or the need for a statement of IRB approval of the research described in that article. Neither did that training prevent her from offering emotional public testimonials regarding the questionable scientific justification for and supposed efficacy of the Geiers’ “Lupron protocol,” or serving on an IRB established and controlled by the principal investigators in the research it purported to supervise—a study in which her son was the first participant.
“Ruggiero is an old hand at this plausibly-deniable Tergiversation Tango, having perfected it with his just-asking-questions Antivax AIDS denial-cake, both eating and f**king it.” – Smut Clyde
Reputable academic journals will not publish articles lacking an assurance that research on human subjects was conducted with IRB approval. Medical Science Monitor’s Instructions for Authors state:
“The MSM editors endorse the principles embodied in the Declaration of Helsinki and expect that all investigations involving humans will have been performed in accordance with these principles. For animal experimentation reported in the journal, it is expected that investigators will have observed the Interdisciplinary Principles and Guidelines for the Use of Animals in Research, Testing, and Education issued by the New York Academy of Sciences’ Adhoc Committee on Animal Research. All human and animal studies must have been approved by the investigator’ Institutional review board.”
In spite of the journal’s policies, “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines” contains no statement regarding IRB approval and supervision. This oversight is especially notable in light of the fact that Medical Science Monitor’s former Editor in Chief (now Editor Emeritus), Prof George B. Stefano, who formerly served as Vice-Chairman of the Research Foundation of the State University of New York (SUNY), a role that should generally require more than a passing familiarity with ethical standards for human subjects research.
[Note: George Stefano, who abandoned his top job in USA to focus on being professor at Charles University Prague in Czechia (it is not clear if he still works there), also used to be chair of the Baord of Durectors at the (now likely defunct) US company MitoGenetics LLC, which claimed to have “found therapeutic solutions for […] type 2 diabetes, obesity, heart disease, hypertension, Alzheimer’s disease and Parkinson’s disease“, using proprietory “therapeutic products to manipulate mitochondria“. I can hear Smut Clyde tutting and chuckling. -LS}.
Medical Science Monitor would become the most prolific disseminator of Mark and David Geier’s litigation-driven outpourings, publishing a total of ten papers between 2004 and 2016. (The runner up is the Polish journal Acta Neurobiologiae Experimentalis, publisher of nine papers by the Geiers between 2009 and 2020.) Prof. Stefano is also Deputy Chief Editor of Neuroendocrinology Letters; he would approve its first article by the Geiers for their August 2006 issue, and would go on to publish a total of five papers by the Geiers in that journal between 2006 and 2014. In sum, Prof. Stefano can be credited with green-lighting a whopping fifteen papers by the Geiers over the course of ten years, even after being warned that large portions of one of the earliest papers they submitted to him for consideration had been plagiarised; even after being warned that their VSD research lacked any statement of IRB approval; and even after widely-publicized sanctions against both authors were issued by the Maryland Board of Physicians.
Geier D, Geier M. A meta-analysis epidemiological assessment of neurodevelopmental disorders following vaccines administered from 1994 through 2000 in the United States.Neuro endocrinology letters (2006); 27(4): 401-413
Frontiers is a somewhat unconventional open access publisher, which likes to have it both ways: playing scientific elite while accepting almost anything from paying customers. My regular contributor Smut Clyde will tell you below how some anti-vaccine scare-mongers managed to sneak in some rather dangerous works thanks to Frontiers’ unofficial “we don’t judge, we just…
In a letter sent to Prof. Stefano on August 8, 2005, and obtained via a FOIA request by this author, Dr. Frank DeStefano of the Centers for Disease Control aired his concern about the similarities between “A two-phased population epidemiological study of the safety of thimerosal-containing vaccines” and the 2000 Verstraeten draft, of which he was a co-author, and to alert him to the lack of any statement of IRB approval for Mark and David Geier’s study.
“Dear Dr. Stefano:
I am the Acting Director of the Immunization Safety Office of the Centers for Disease Control and Prevention (CDC). I am writing to express my concerns about the source of some of the material in a recent article published in Medical Science Monitor that purposed to analyze data from the Vaccine Safety Datalink (VSD), a project that is located within my office. Specifically, the article by Geier and Geier, “A Two-Phased Population Epidemiologic Study of the Safety of Thimerosal-Containing Vaccines: A Follow-Up Analysis,” appearing in the April issue (Med Sci Monit 2005;11: CR160-170) contains striking similarities between parts of the article, including nearly all of the results from the “Phase II” study, and a draft manuscript on which I am co-author.
In the article, Geier and Geier state that as independent researchers they have analyzed data on a cohort of children in the VSD database (see page CR163 of the article) and the paper is written to indicate that they themselves performed these analyses. Much of the text and the “Phase II” results in their article are nearly identical to a draft manuscript written in June 2000 by Thomas Verstraeten, Robert Davis, and myself for the VSD investigators. This was the first draft of a study whose final results were ultimately published in Pediatrics in November 2003 (reference #29 in the Geier and Geier article). The VSD June 2000 draft manuscript was based on preliminary results presented at the meeting of the Advisory Committee on Immunization Practices that month. The draft manuscript was obtained by the advocacy group Safe Minds in 2001 through the Freedom of Information Act and is posted on their website at the following link: http://www.SafeMinds.org/legislation/foia/VSD_VerstraetenJune2000.pdf.
I have enclosed copies of both the Geiers’ published article and the June 2000 VSD draft manuscript (as downloaded directly from the publicly-accessible Safe Minds website) for your review. I have highlighted with similar colors those sections and results in the two documents that are the same. As you will note, in the “Phase II” results section of the published article the Geiers report the same relative risks as those that are found in the VSD June 2000 draft manuscript (Table 3, Page 9). Also, Table 4 and Table 5 in the Geier article contain exactly the same results as Table 1 (page 6) and Table 2 (page 7), respectively, in the VSD draft manuscript. Furthermore, the text in several sections of the Geier article is nearly identical to corresponding sections of the VSD June 2000 draft manuscript.
I also have doubts that the Geiers actually performed the “Phase II” analyses because to the best of my knowledge they have not had access to the VSD data required to perform those analyses. I could provide more details if you like.
I felt it was important to inform you of this situation since you may not have been aware of the previous work by the CDC. I hope that you will be able to carefully review the circumstances surrounding the Geier article for its ethical implications and compliance with your journal’s policies of authorship.
Sincerely yours,
Frank DeStefano MD MPH”
Although an editorial staff member of Medical Science Monitor acknowledged receipt of Dr. DeStefano’s letter on August 17, 2005, neither Prof. Stefano nor the journal’s Editorial Board appear to have ever responded further.
Another manuscript by Mark and David Geier was received by Medical Science Monitor on August 8, 2005 (the same day that Dr. DeStefano sent his letter), accepted on February 28, 2006, and eventually published in the journal’s June 2006 issue.
David A Geier, Mark R Geier An assessment of downward trends in neurodevelopmental disorders in the United States following removal of Thimerosal from childhood vaccinesMedical Science Monitor (2006) Jun;12(6):CR231-9.
The similarities between that article and another paper by the Geiers, which was published in the Spring 2006 issue of the Journal of American Physicians and Surgeons, are as striking as those described here.
David A Geier, Mark R Geier Early downward trends in neurodevelopmental disorders following removal of thimerosal-containing vaccinesJournal of American Physicians and Surgeons (2006) Spring:1(11):8-13
Another instalment of grifting quackery in COVID-19 pandemic. Cedars-Sinai scientists and their biotech partners Aytu Biosciences want to light you up from inside, just as President Trump suggested.
The Geiers’ unattributed appropriation of the work of Verstraeten, De Stefano, et al., was not limited to their Two-Phased Study, and continued to at least 2012.
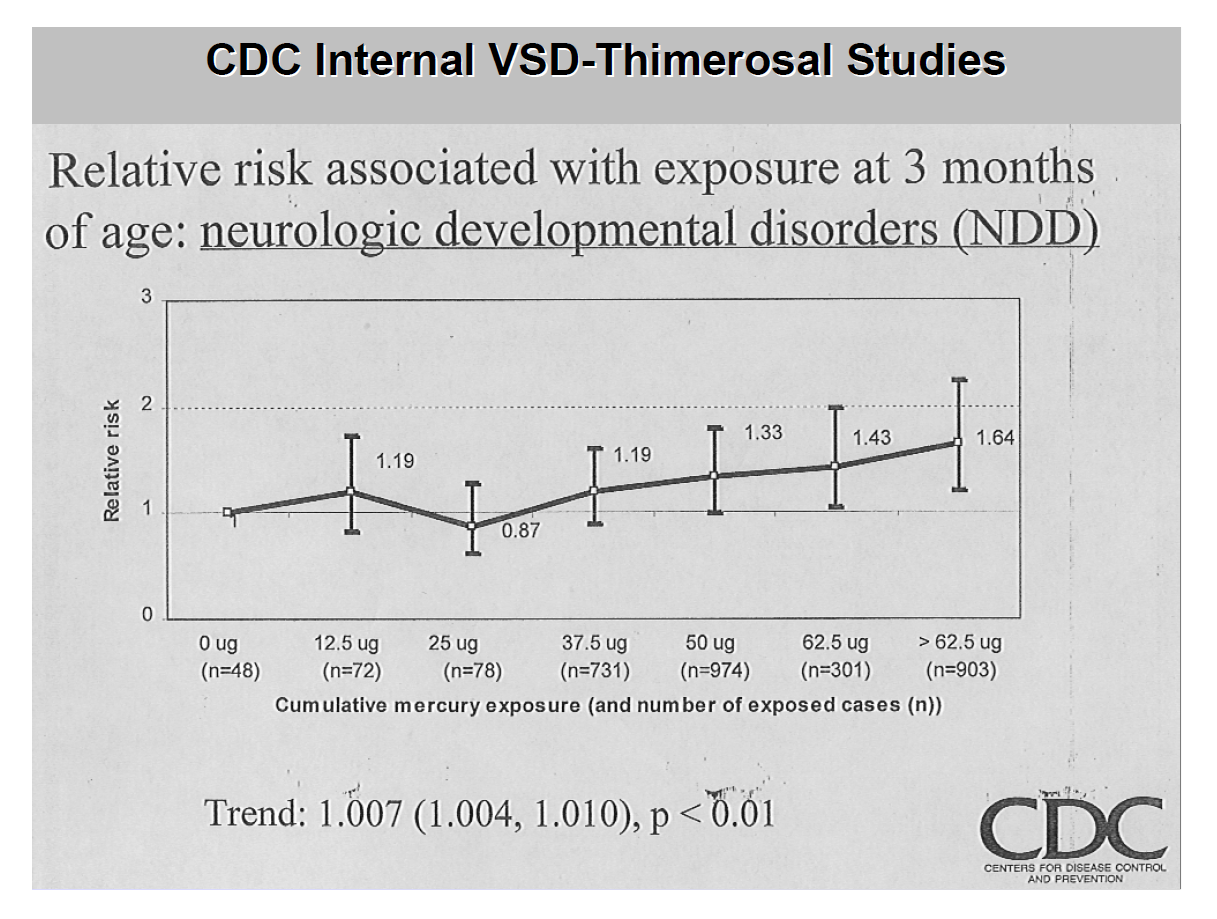
Their 2012 Powerpoint slide deck, “An Overview of the History of Thimerosal (Mercury),” features a graph copied from the 2000 Verstraeten draft, then altered to omit relevant text, and to add the CDC logo.
“CDC Internal VSD-Thimerosal Autism Studies” graph on page 40 of the Geiers’ 2012 slide deck
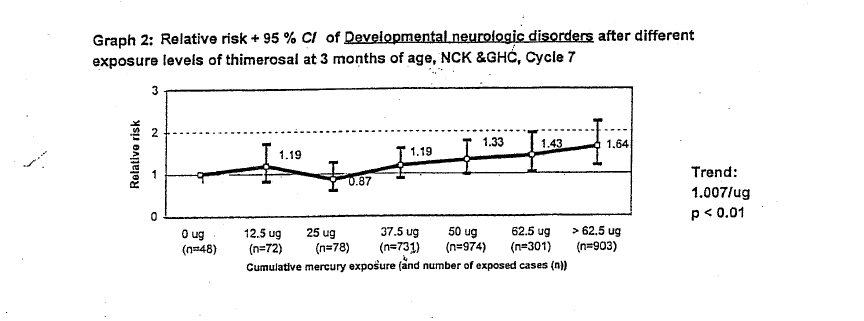
Note that Graph 2 of the 2000 Verstraeten draft uses a sans-serif font, whereas the text at the top and bottom of the Geiers’ slide uses a serif font. The header on the Geiers’ slide reads, “Relative risk associated with exposure at 3 months of age: neurologic developmental disorders (NDD)”. This header omits data from the header above Graph 2 in the 2000 Verstraeten draft, which reads, “Graph 2: Relative risk + 95 % CI of Developmental neurologic disorders after different exposure levels of thimerosal at 3 months of age, NCK & GHC, Cycle 7“.
The graph number, the confidence interval, the kind of exposure, the sources (Northern California Kaiser and Group Health Cooperative), and the cycle were all omitted. The word order of “Developmental neurologic disorders” was changed to “neurologic developmental disorders” and the abbreviation “NDD” was added, which appears nowhere in either the draft or Verstraeten’s final report.
The text at the bottom of the Geier slide reads, “Trend: 1.007 (1.004, 1.010), p <001″. This is a direct transcription of the text to the right of Graph 2, to which was added “(1.004, 1.010)“.
The Geiers’ slide features the CDC’s logo at the bottom right hand corner, a misleading modification implying that the graph was an official, final publication of the CDC. The CDC logo appears nowhere in the Verstraeten draft, or in the finished paper.
Although the slide deck in which this graph appears was created in March 2012, it is likely that Mark and David Geier poached it from the 2000 Verstraeten draft when they originally became aware of its existence. In fact, the Geiers’ slide appears to have been created from a well-worn photocopy of a sloppy analog cut-and-paste job, created by someone with little skill at image editing.
Mark & David Geier “An Overview of the History of Thimerosal (Mercury)” (2012) Powerpoint slide deck
Recommended reading on Mark and David Geier
Jessica Steir, “The playbook used to ‘prove’ vaccines cause autism” (New York Times, August 19, 2025)
Tom Bartlett, “You could throw out the results of all these papers” (The Atlantic, July 23, 2025).
Liz Weil, “The father-son duo who toppled trust in vaccines” (New York Magazine, July 17, 2025).
Liz Essley Whyte and Dominique Mosbergen, “Vaccine opponent hired by RFK Jr. scours official records for link to autism” (Wall Street Journal, June 5, 2025).
Brandy Zadrozny, “The little-known database at the heart of Kennedy’s vaccine conspiracy theory” (NBC News, April 30, 2025).
Smut Clyde, “The Dead Geier Sketch, RFK Jr version” (For Better Science, April 7, 2025).
David Gorski, “David Geier: A blast from the antivax past hired to “prove” vaccines cause autism” (Respectful Insolence, March 26, 2025).
Trine Tsouderos, “Miracle drug called junk science” (Chicago Tribune, May 21, 2009).
If you are interested to support my work, you can leave here a small tip of $5. Or several of small tips, just increase the amount as you like (2x=€10; 5x=€25). Your generous patronage of my journalism will be most appreciated!
RFK Jr. and his fellow anti-vaxers threaten to turn the USA into a bastion of pseudoscience, not unlike the Lysenko fiasco in Russia under Stalin and Khrushchev. This is the problem with mixing politics and science too deeply. Will opposing American scientists be sent to Trump’s detention centers, or is cutting off federal funding achieving the same goal? Can’t wait until this administration is gone.
I think, egle, that you underestimate the extent of the problem, which did not appear (and will not simply disappear) with Trump and his entourage. This is a larger problem that involves a long-entrenched identity politic enabled and accelerated by technology (for example, social media). Though it appears to be the headline, it is but a symptom of something larger.
I agree that social media is a big part of the problem. But the Trump administration has moved the fringe element into the mainstream of power. Their attacks to cripple institutions like higher ed, NIH, EPA, FEMA, NOAH, CDC etc. may never be reversed the longer they control the government.
I wrote a long and, I thought, clever comment comparing the Geiers’ fake science to the problem of students using AI to pretend they understand the material in their classes, and then some kind of website hiccup disappeared it. Anyway, thank you Kathleen for this infuriating piece.




















RFK Jr. and his fellow anti-vaxers threaten to turn the USA into a bastion of pseudoscience, not unlike the Lysenko fiasco in Russia under Stalin and Khrushchev. This is the problem with mixing politics and science too deeply. Will opposing American scientists be sent to Trump’s detention centers, or is cutting off federal funding achieving the same goal? Can’t wait until this administration is gone.
LikeLiked by 2 people
Agreed. They are cynical, inhumane, and criminally misinformed and short-sighted
LikeLiked by 2 people
I think, egle, that you underestimate the extent of the problem, which did not appear (and will not simply disappear) with Trump and his entourage. This is a larger problem that involves a long-entrenched identity politic enabled and accelerated by technology (for example, social media). Though it appears to be the headline, it is but a symptom of something larger.
LikeLiked by 1 person
I agree that social media is a big part of the problem. But the Trump administration has moved the fringe element into the mainstream of power. Their attacks to cripple institutions like higher ed, NIH, EPA, FEMA, NOAH, CDC etc. may never be reversed the longer they control the government.
LikeLiked by 2 people
I wrote a long and, I thought, clever comment comparing the Geiers’ fake science to the problem of students using AI to pretend they understand the material in their classes, and then some kind of website hiccup disappeared it. Anyway, thank you Kathleen for this infuriating piece.
LikeLiked by 2 people
You’re welcome. It’s all so outrageous, not only the Geiers’ mendacity, but the editor’s enablement.
LikeLiked by 2 people