
Coronavirus COVID-19 pandemic is about to be stopped by a stroke of a French “genius” with a history of publishing manipulated data. The charismatic Didier Raoult, director of the Research Unit in Infectious and Tropical Emergent Diseases (URMITE) in Marseille has found a cure: the humble chloroquine, cheap unpatented substance used to treat malaria and autoimmune diseases lupus and rheumatism. The substance so far failed in all antiviral therapies, but this didn’t prevent Raoult from deciding that chloroquine can cure corona virus infections, serious side effects notwithstanding. To prove that, Raoult treated 26 patients at his institution with the derivative hydroxychloroquine, alone and in combination with the antibiotic (meaning antibacterial!) drug azithromycine. The study was not randomised, ethically approved only after it already began, and it was not really controlled: the 16 control patients were treated in different clinics.
After some adjustments (patients removed, data points guessed), a preprint was published simultaneously with a paper in a peer reviewed journal Raoult basically controls. Next, a lawyer with whom Rault partnered with pitched the miracle cure to Fox News, which is the TV channel US president Donald Trump watches all day to get all his information. Trump then tweeted this:
Chaos ensued. People worldwide stormed pharmacies and pet shops for chloroquine, some killed themselves with aquarium cleaner, India banned chloroquine export, while national authorities including French government decided to deploy chloroquine as the medicine to treat COVID19. All based on Trump’s tweets which in turn was based on Fox News promotion of this study by Raoult:
Philippe GAUTRET , Jean Christophe LAGIER  , Philippe PAROLA , Van Thuan HOANG , Line MEDDED , Morgan MAILHE , Barbara DOUDIER , Johan COURJON , Valerie GIORDANENGO , Vera ESTEVES VIEIRA , Herve TISSOT DUPONT , Stephane HONORE , Philippe COLSON , Eric CHABRIERE , Bernard LA SCOLA , Jean Marc ROLAIN , Philippe BROUQUI , Didier RAOULT Hydroxychloroquine and Azithromycin as a treatment of COVID-19: preliminary results of an open-label non-randomized clinical trial medRxiv (2020) doi: 10.1101/2020.03.16.20037135 and International Journal of Antimicrobial Agents (2020) doi: 10.1016/j.ijantimicag.2020.105949
, Philippe PAROLA , Van Thuan HOANG , Line MEDDED , Morgan MAILHE , Barbara DOUDIER , Johan COURJON , Valerie GIORDANENGO , Vera ESTEVES VIEIRA , Herve TISSOT DUPONT , Stephane HONORE , Philippe COLSON , Eric CHABRIERE , Bernard LA SCOLA , Jean Marc ROLAIN , Philippe BROUQUI , Didier RAOULT Hydroxychloroquine and Azithromycin as a treatment of COVID-19: preliminary results of an open-label non-randomized clinical trial medRxiv (2020) doi: 10.1101/2020.03.16.20037135 and International Journal of Antimicrobial Agents (2020) doi: 10.1016/j.ijantimicag.2020.105949
It is the opposite of proper clinical research practice. The trial started somewhere in March, likely before an ethics vote was applied for. But already on 11 February 2020 Raoult and colleagues decreed which drug can prevent and cure COVID-19. They wrote about chloroquine in Colson et al 2020, published in the same journal:
“Hence, its possible use both in prophylaxis in people exposed to the novel coronavirus and as a curative treatment will probably be promptly evaluated by our Chinese colleagues.”
Normally, Raoult demands that “Studies of infectious syndromes should no longer be mined without consistently using negative controls to assess the positive predictive value of a positive result.” This he obviously does not apply to himself, especially when the clinical result is already decided in advance. In his own research, Professor Raoult is no fan of randomised controlled clinical trials. A PubPeer user translated his interview:
As Elisabeth Bik discussed, the paper was peer-reviewed in less than 24h, it probably helped that the journal’s Editor-in-Chief is both the paper’s coauthor and Raoult’s IHU subordinate Jean-Marc Rolain. Bik also listed other problems with that paper. Like this:
“In the EU Clinical Trial Register page, the study was described as evaluating PCR data on Day 1, Day 4, Day 7 and Day 14. However, the study show the data for Day 6, which is different than planned. Why did the authors not show the results on Day 7? Did the data on day 7 not look as good?”

In fact, the authors never showed the results of day 14 either. They also refused to share their secondary endpoint data, namely “the clinical effectiveness of treatment on time to apyrexia, normalization of respiratory rate, and average length of hospital stay and mortality”. Basically, it is none of anyone’s business to know if the therapy had any clinical benefit for the patients.
Noteworthy, the control patients were much younger than the treated ones. Which is convenient since COVID19 is generally not dangerous to younger persons. The average age of the control group was 37, that of hydroxychloroquine-treated group 53 years old. Also, as Bik noted:
“The [hydroxychloroquine] treated patients were all in Marseille, while the controls were located in Marseille or other centers.”
Even then, additional tricks were apparently needed. Viral load in control patients was analysed by quantitative RT-PCR and a bit too liberally, as Bik explains:
“Of particular note, control patients 6 and 8-16 appear to have been analyzed differently. Their Day 0 PCR values are not given as CT values (the number of cycles after which a PCR becomes positive, the lower the number, the more virus is present) but as POS/NEG, suggesting a different test was used. […] Several patients in the control group did not even have a PCR result on Day 6, so it is not clear how they were counted in the Day 6 result.”

Some control patients were tested only every second day, afterwards guessed to be positive, some were not tested at all on day 0, as a PubPeer commented noted. And then the authors simply changed the results in control patients between the “in press” and the final paper version, as another PubPeer uses observed:
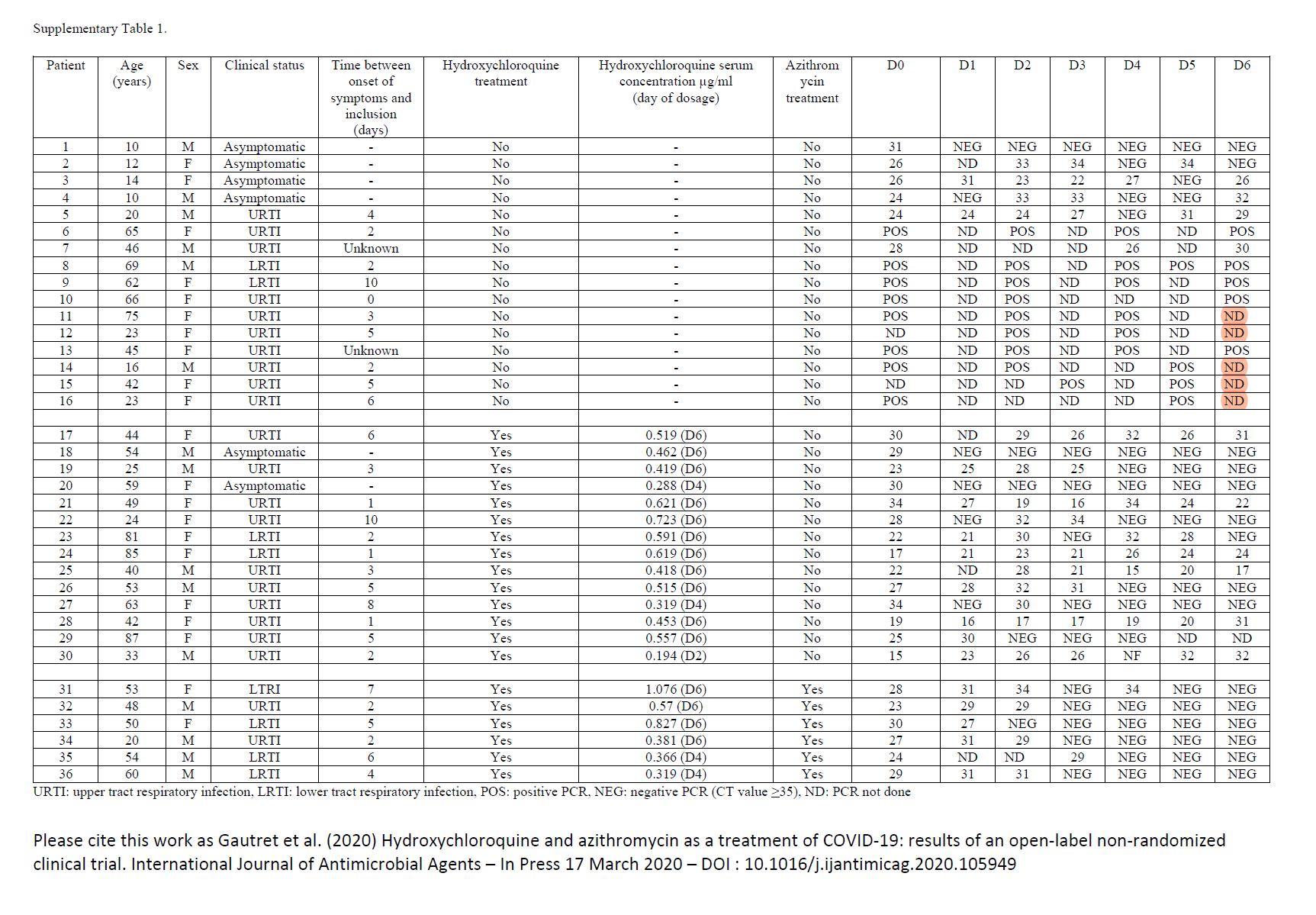
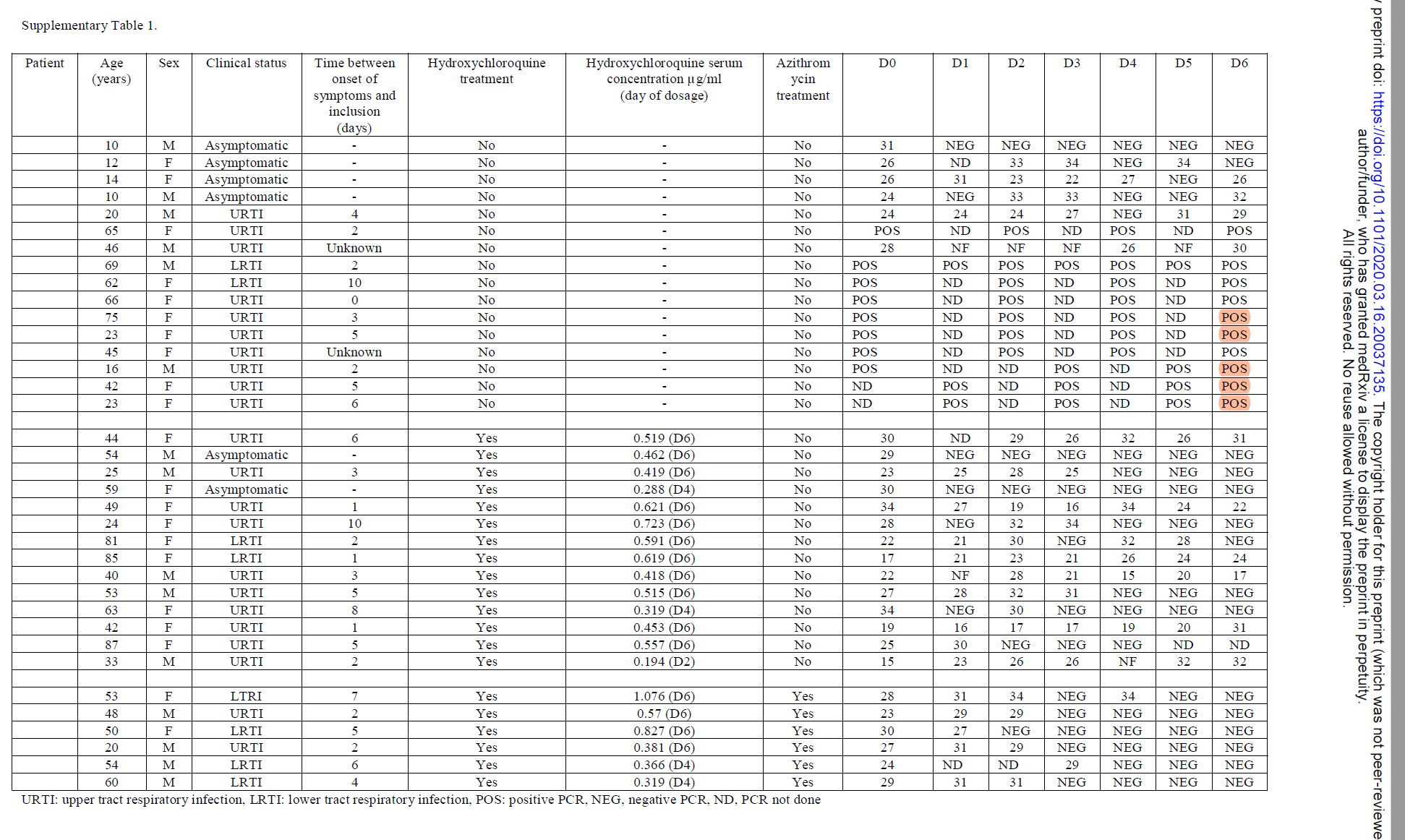

Another PubPeer user re-ran the analysis, because “an important number of non-treated patients were not tested by PCR (ND)“. Once the ND values were disregarded, there wasn’t any more significant difference between controls and chloroquine-treated patients.
Not only control group had to be adjusted: the treatment group somehow lost 6 patients, as Bik discussed:
“Although the study started with 26 patients in the HQ or HQ+AZ group, data from only 20 treated patients are given, because not all patients completed the 6-day study. The data for these 20 patients looks incredibly nice; especially the patients who were given both medications all recovered very fast.
What happened to the other six treated patients? Why did they drop out of the study? Three of them were transferred to the intensive care unit (presumably because they got sicker) and 1 died. The other two patients were either too nauseous and stopped the medication, or left the hospital […] So 4 of the 26 treated patients were actually not recovering at all.”
It seems, the authors simply removed inconvenient patients from the analysis before publishing their study. They left online their previous evaluation though, which showed a slightly different result, compare here the day 6 time point:

Statistical and ethical problems with that Gautret et al 2020 study were addressed extensively in this preprint by Dahly, Gates & Morris zenodo 2020. The authors also reject Raoult’s claims about previous positive results from China:
“In the background of their paper, Gautret et al referred to “an early clinical trial conducted in COVID-19 Chinese patients, [which] showed that chloroquine had a significant effect, both in terms of clinical outcome and viral clearance, when comparing to control groups”. There were two citations for this claim. The first was a letter7 that doesn’t report any trial data, but instead refers to a conference held in China in February, during which participants (“experts from government and regulatory authorities and organizers of clinical trials”) seemingly agreed that chloroquine was an efficacious treatment for COVID-19. The second cition (also included in the aforementioned letter) refers to a number of clinical trials registered in China, though many of these have now been suspended or closed, while the remaining trials are still recruiting (per their entries on http://www.chictr.org.cn as of March 21, 2020). Hence there are, to our knowledge, no other published reports of clinical trials testing the efficacy of chloroquine for COVID-19 treatment.”

However, now a proper randomised controlled clinical trial was done in China on chloroquine treatment of COVID19. The authors of Chen et al 2020 report:
“One patient in HCQ group developed to severe during the treatment. On day 7, COVID-19 nucleic acid of throat swabs was negative in 13 (86.7%) cases in the HCQ group and 14 (93.3%) cases in the control group (P>0.05). The median duration from hospitalization to virus nucleic acid negative conservation was 4 (1-9) days in HCQ group, which is comparable to that in the control group[2 (1-4) days, (U=83.5, P>0.05)]. The median time for body temperature normalization in HCQ group was 1 (0-2) after hospitalization, which was also comparable to that in the control group 1 (0-3). Radiological progression was shown on CT images in 5 cases (33.3%) of the HCQ group and 7 cases (46.7%) of the control group, and all patients showed improvement in follow-up examination. Four cases (26.7%) of the HCQ group and 3 cases (20%) of the control group had transient diarrhea and abnormal liver function (P>0.05)”

BUT WHAT IF RAOULT IS RIGHT AND IT WORKS?????
I hear you ask that. After all, Raoult is a star of French science: he publishes a scientific paper “nearly every work day”, thanks to 800 employees working under him, as a blog post mentioned, and he is so important that his Marseille collaborators named two bacteria species after the grand director: Raoultella planticola and Rickettsia raoultii.
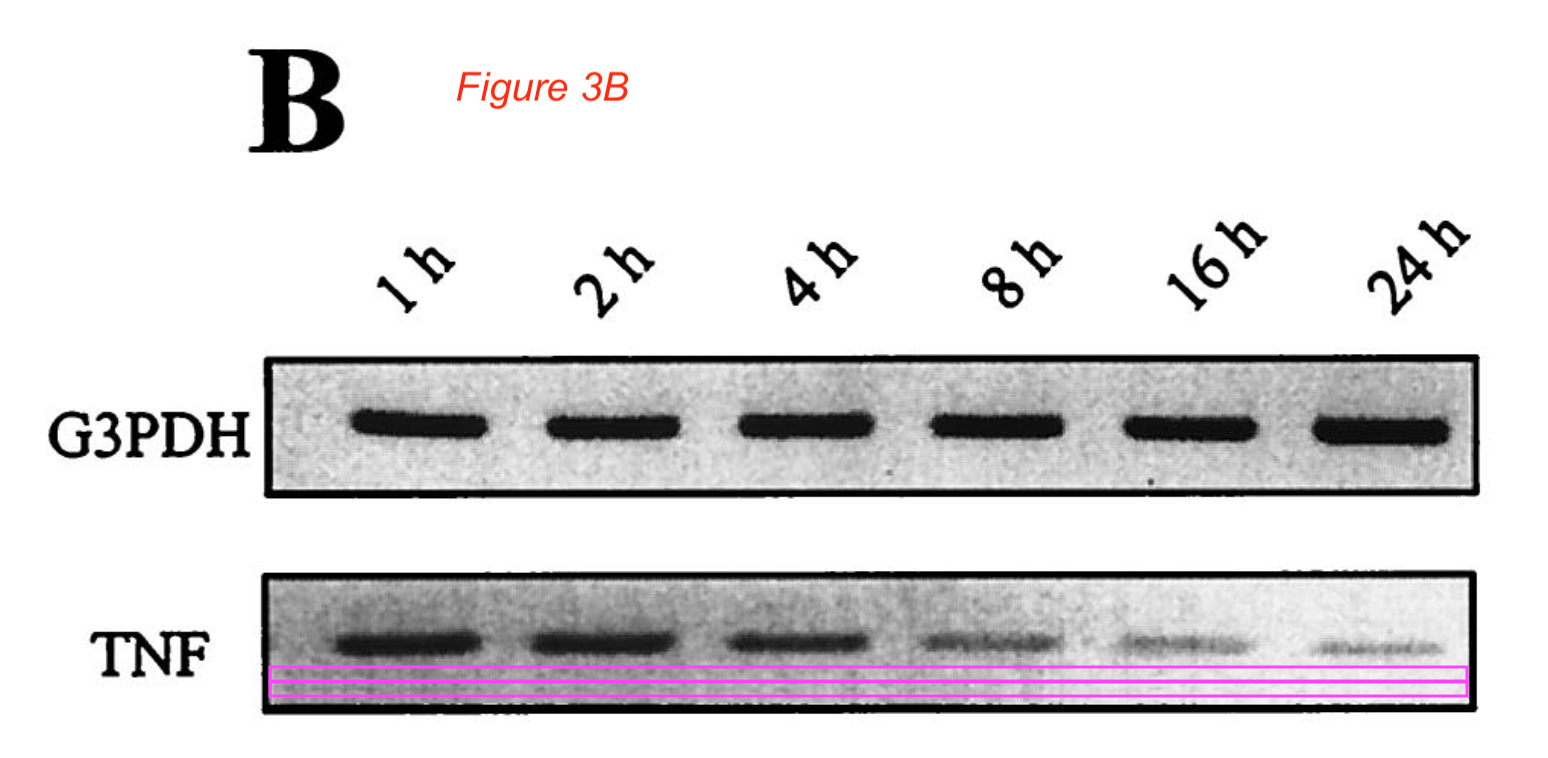
Well, Elisabeth Bik found some very bad data fakery in a 15 year old Raoult-co-authored paper:
Florence Fenollar , Stéphane Sire , Nathalie Wilhelm , Didier Raoult Bartonella vinsonii subsp. arupensis as an agent of blood culture-negative endocarditis in a human Journal of Clinical Microbiology (2005)
doi: 10.1128/jcm.43.2.945-947.2005

The gels are most obviously fake, falsified in Photoshop. In at least one instance, a gel band was erased digitally. Here a younger Raoult-coauthored paper from URMITE Marseille, and it is not much better:
Miguel A. De La Cruz , Weidong Zhao , Carine Farenc , Grégory Gimenez , Didier Raoult , Christian Cambillau , Jean-Pierre Gorvel , Stéphane Méress A toxin-antitoxin module of Salmonella promotes virulence in mice PLoS Pathogens (2013) doi: 10.1371/journal.ppat.1003827
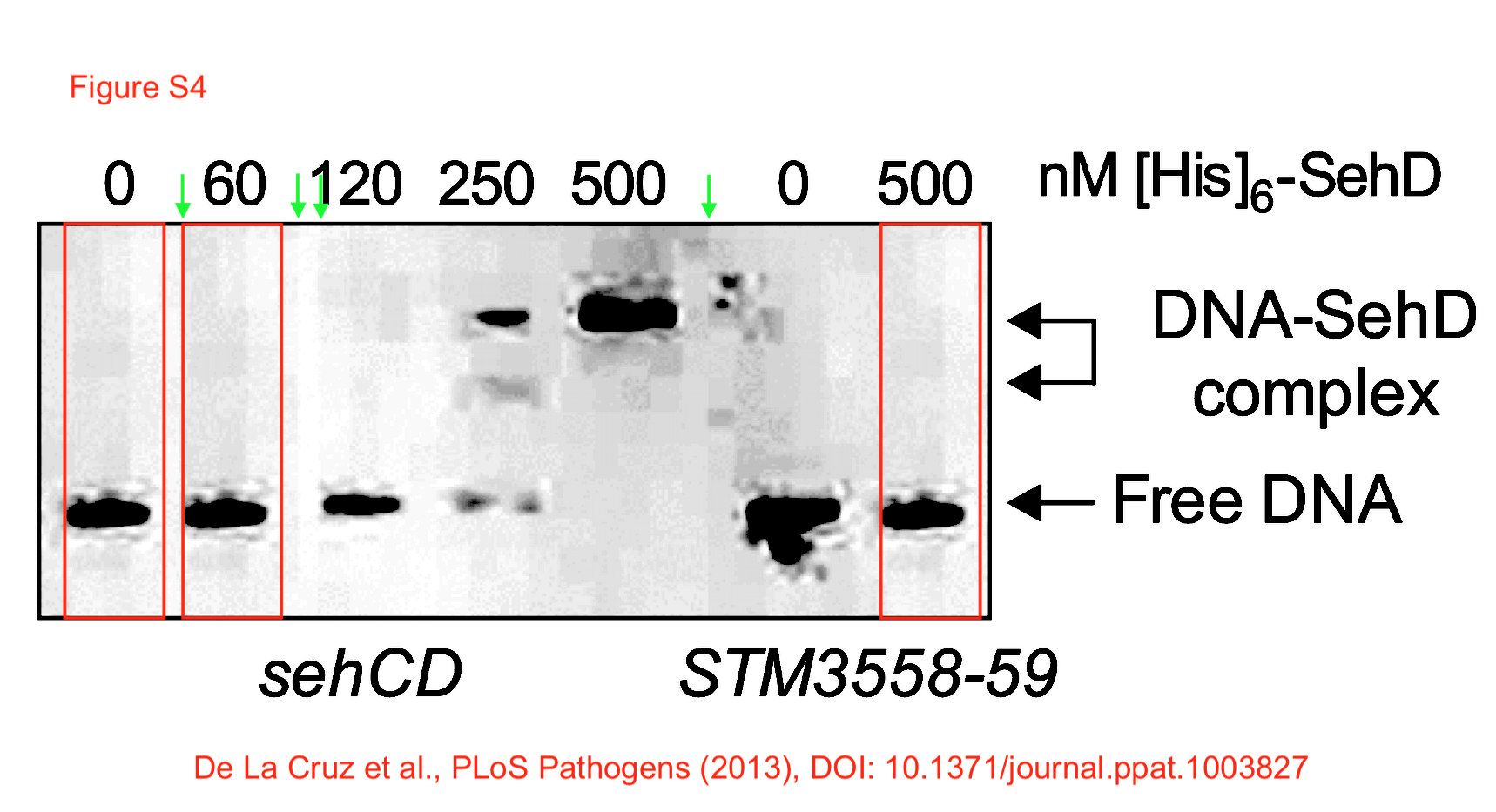
A gel lane was copied three times, while arrows indicate additional image manipulations in that gel figure. The last author Stéphane Méresse seems not to deny that the image was fabricated:
“This image should never have been published and we apologize for this mistake. Below two similar experiences leading to the same conclusion.”
Caught on fake data? Replace it with something else, conclusions not affected. As easy as removing patients from analysis or guessing PCR results. The research culture at URMITE produced also this beauty, again with Raoult as coauthor:
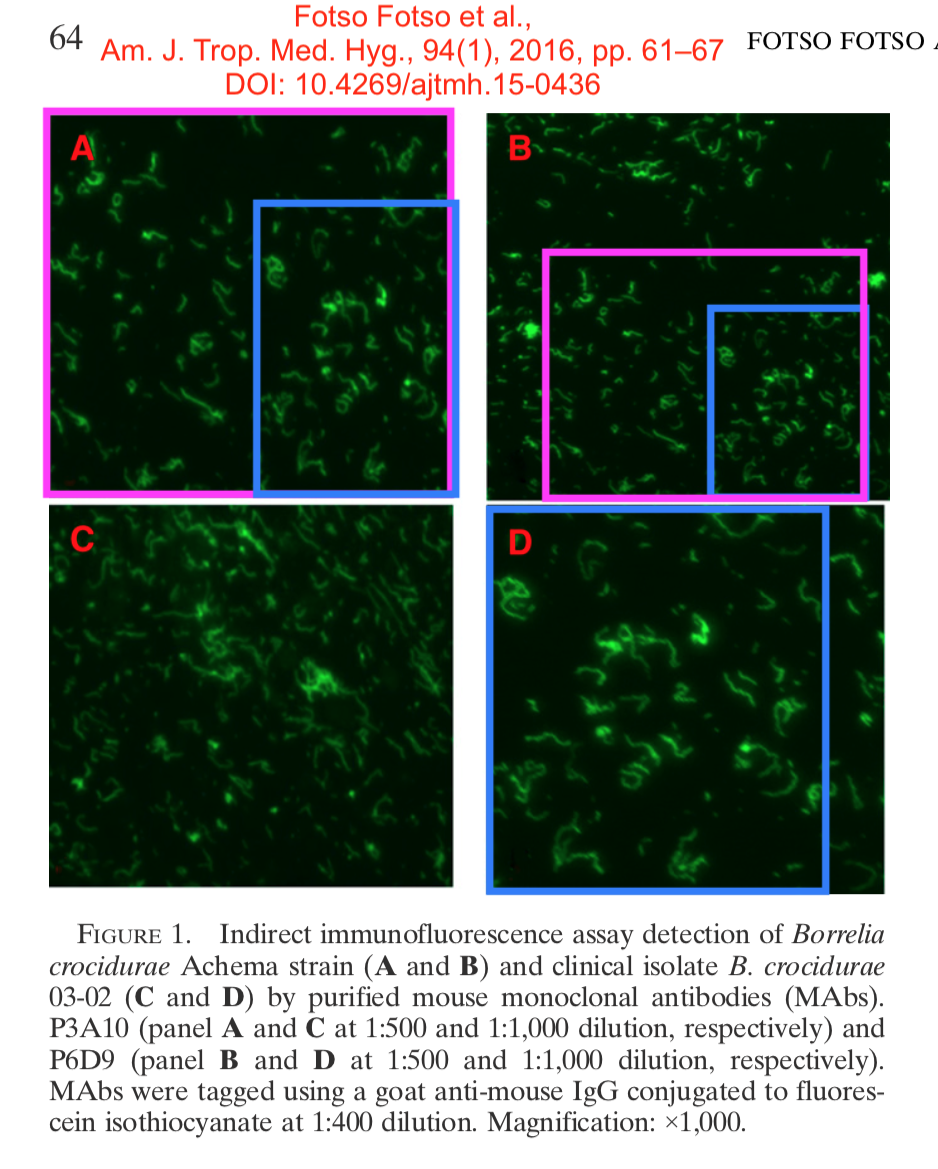
Aurélien Fotso Fotso , Oleg Mediannikov , Didier Raoult , Claude Nappez , Michel Drancourt , Michel Azza Monoclonal Antibodies for the Diagnosis of Borrelia crocidurae American Journal of Tropical Medicine and Hygiene (2016) doi: 10.4269/ajtmh.15-0436
That is truly a beautiful fake. Fractal bacteria, as someone commented on Twitter. Bik found also this, a 19 year old microscopy collage co-authored by Raoult:
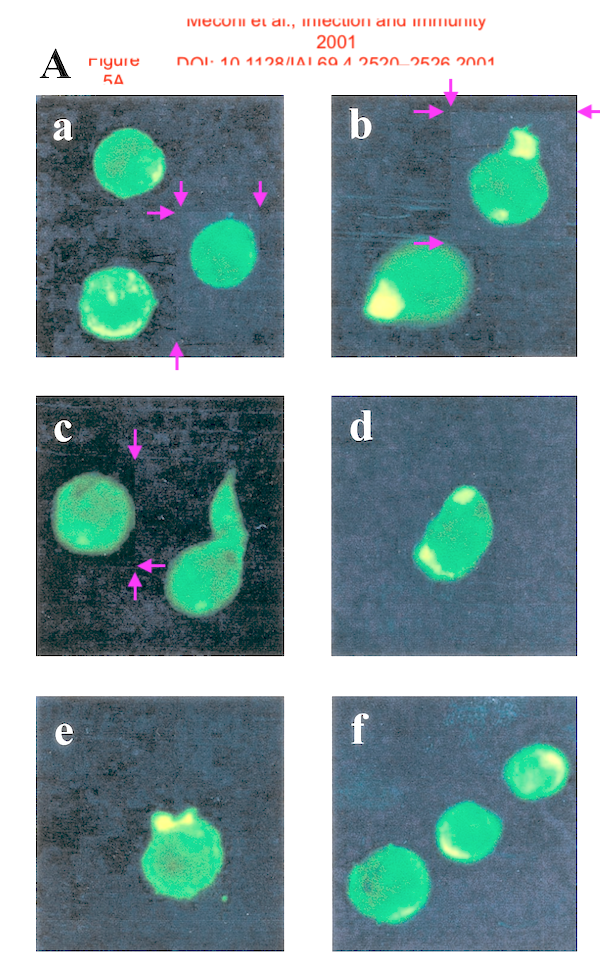
S Meconi , C Capo , M Remacle-Bonnet , G Pommier , D Raoult , J L Meg Activation of protein tyrosine kinases by Coxiella burnetii: role in actin cytoskeleton reorganization and bacterial phagocytosis Infection and Immunity (2001) doi: 10.1128/iai.69.4.2520-2526.2001
The arrows indicate that the cells were digitally pasted in. To catch Raoult on having published fabricated data is not really a surprise, as it turned out.
More recently, Raoult’s lab simply slightly darkened an image of a 2D western blot and re-used it again, for a different bacteria. Nobody complained.
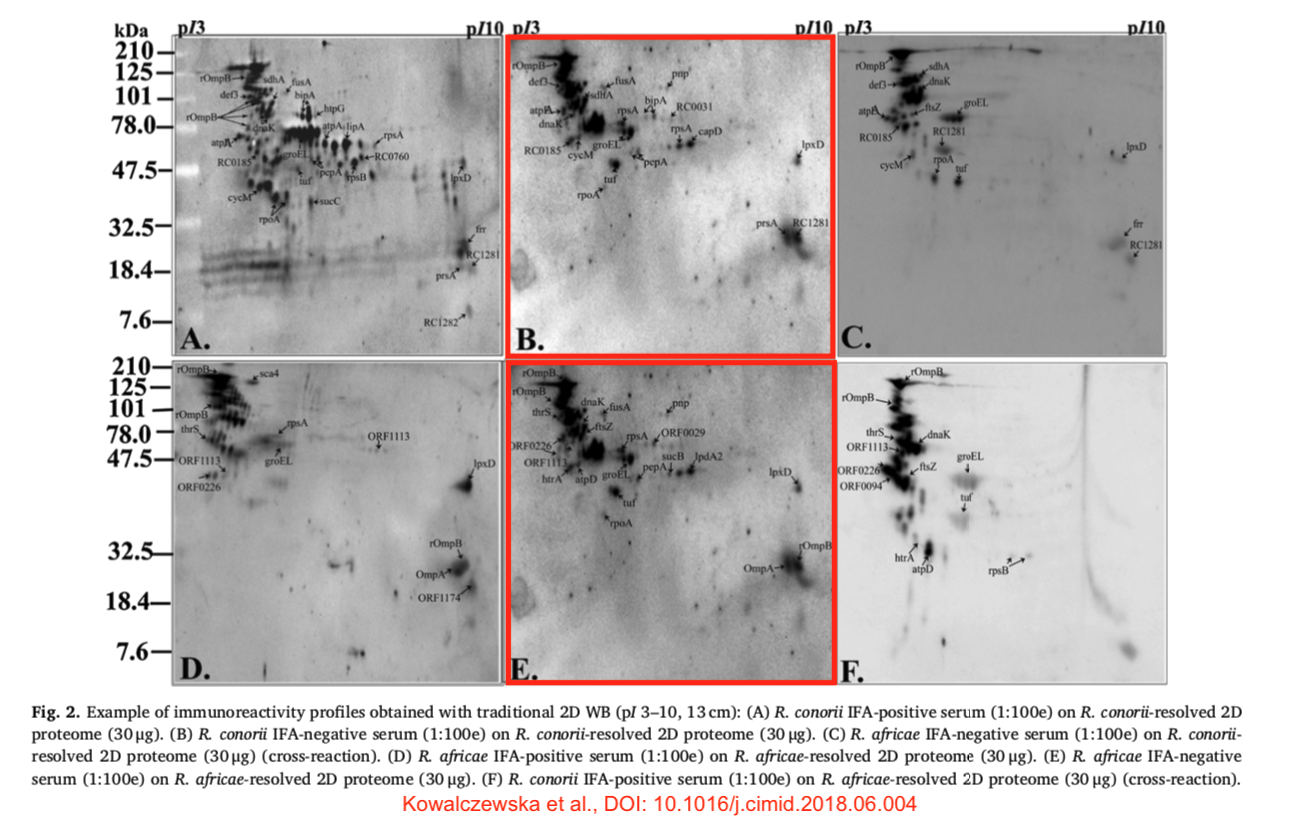
M Kowalczewska, A N’Djatchi , C Nappez , S Alwassouf, P Decloquement, N Armstrong, K El Karkouri, S Edouard, D Raoult Identification of rickettsial immunoreactive proteins using a proximity ligation assay Western blotting and the traditional immunoproteomic approach Comparative Immunology Microbiology and Infectious Diseases (2018) doi: 10.1016/j.cimid.2018.06.004
Other PubPeer users joined Bik on the treasure hunt and found another duplicated gel, again slightly darkened:
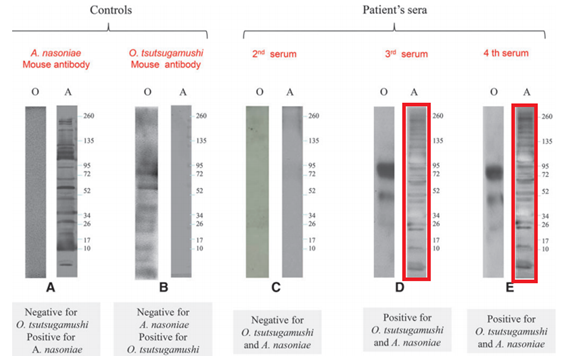
S Edouard , G Subramanian , B Lefevre , A Dos Santos , P Pouedras , Y Poinsignon , O Mediannikov , D Raoult Co-infection with Arsenophonus nasoniae and Orientia tsutsugamushi in a traveler Vector-Borne and Zoonotic Diseases (2013) doi: 10.1089/vbz.2012.1083
In 2012, Science magazine brought an article about Raoult’s scientific achievements, where hidden among all the celebration were descriptions of his bullying and lack of basic research integrity. Some quotes:
“Yet Raoult is also known for his enmities and his disdain for those who disagree with him. “People don’t like to talk about him because he has a lot of influence. He can make life hard for you,” says one of several French researchers contacted by Science who would only talk about Raoult if they could remain anonymous. “Few of his science colleagues will find the thought of another profile story about him particularly appealing,” geneticist Jean-Michel Claverie of Aix-Marseille University—who severed ties with Raoult in 2006 after a 5-year collaboration—wrote in an e-mail to Science“.
and then:
“But some scientists grumble that manuscripts out of Raoult’s lab often contain errors, for instance, as a result of unchecked genetic sequences.
Indeed, problems in a paper about a mouse model for typhus got his lab in hot water in 2006. A reviewer for Infection and Immunity, a journal published by the American Society for Microbiology (ASM), discovered that four figures in a revised manuscript were identical to figures in the original manuscript, even though they were supposed to describe a different experiment.
In letters to ASM, made available by Raoult, second author Christian Capo and last author Jean-Louis Mège, a group leader, accepted “full responsibility” for the problem, which they said involved only two figures. Capo, in his letter, wrote that he had made an innocent mistake; Mège wrote that Capo had subsequently failed to show the revised manuscript to other authors, who were on vacation, before resubmitting it. But after consulting its ethics panel, ASM banned all five authors, including Raoult, from publishing in its journals for a year. “We are not entirely comfortable with the explanation provided,” ASM officials wrote to Mège. “Misrepresentation of data … is an affront to the ethical conduct of scientific inquiry.”
Capo and Mège accepted the decision, but Raoult wrote ASM that he wasn’t at fault and that the “collective punishment” was “very unfair.” He appealed the ban, also on behalf of two other co-authors, but lost. Furious, he resigned from the editorial board of two other ASM journals, canceled his membership in the American Academy of Microbiology, ASM’s honorific leadership group, and banned his lab from submitting to ASM journals, in which he had published more than 230 studies. His name has been on only two ASM journal papers since, both published in 2010. To clear his name, Raoult sent his ASM correspondence to French colleagues in 2007, along with a letter defending himself. “If I had been in the United States, I would have sued,” he wrote.”
Raoult did not like Science coverage of his genius. He made the journal publish an Erratum, where he even wrongly accused the author of shilling for Danone:
“IT WAS AN HONOR TO HAVE MY PROFILE PUBlished in Science (“Sound and fury in the microbiology lab,” C. Mary, News Focus, 2 March, p. 1033). However, I was surprised that 20% of the article is devoted to the American Society for Microbiology (ASM) story, in which I was a collateral victim of a collective sanction (there has been no collective liability in France since World War II). I did not manage the paper and did not even check the last version. The mistake by C. Capo consists of a single figure inversion (not four, as stated in the Science profile). This paper has since been published (1). In January 2007, I was awarded one of the highest ASM honors—the ICAAC lecture—thus clearing doubts about my scientific integrity.”
Accusing your critics of being Nazis or Nazi collaborateurs is standard practice in French academia, especially when you are called out on data manipulation. But you probably started to get a gist that Raoult is not a nice man and not prepared to be criticised or disagreed with. He has a way to make his subordinates deliver the results he likes:
Now, the extra bit of irony is that Raoult is so full of himself that he published in 2018 an opinion piece to teach France some… research integrity. The occasion was the Catherine Jessus affair which I myself incidentally have caused.
Il pleut de la merde
In 2017, Raoult’s leadership was challenged by a sexual harassment and assault scandal at his URMITE institute, an affair with at least six victims which the director himself described as “a love story gone wrong“. The perpetrator was eventually sacked, but Raoult did not handle the case exemplary, quite the opposite. This article in MarsActu narrates that Raoult tried to hush up the affair for two years while even trying to have the victim sacked:
“For CGT union which made public the sanction at a press conference on Monday, these behaviours are not the result of misconduct of a single person but fall under a system set up around the personality of Director URMITE, Didier Raoult. “I am appalled by the fact that the director of the URMITE could not report acts of harassment to his superiors and his guardianship for two years” . […] “The alleged victims and the person they have named as their attacker were installed in adjacent laboratories within the new premises of the IHU” […] “threats (…) currently uttered by Mr. Raoult against Mrs. A, “ . “We have just been informed that Mr. Raoult intends to fire Mrs. A from URMITE. This is unacceptable “ .
Allegedly Raoult also threatened the other victim, a foreign graduate student, warning her that she will not be allowed to complete her thesis if she blows the whistle. Raoult rejected all accusations against himself and denied responsibility. In reality, the gigantic institute is run as his own private fiefdom, as a 2015 evaluation report criticised (discussed in this blog post). Harassment and abuse of students and employees used to be apparently normal under Raoult iron rule, as a 2017 union report criticised:
“Several students or former students testified to work hours without limits, aggravated work stress, work at night or on weekends. They seem to have an enormous pressure for results. Their presence on publications appears to be based on the needs of those responsible. A visit of the CHSCT helped to highlight the fact that, hitherto, lab coats were not provided to them, so they had to get one on their own and had to wash it outside, despite handling of pathogens in the laboratory. […]
We know of many transfer requests, made by the ITA, but also researchers, INSERM, CNRS and Aix-Marseille University. This seems not to have alerted the leadership on the situation of employees in the unit.
The head of the graduate school had to manage a significant number of students from reallocations of URMITE to other units, during or at the end of their thesis.”
Employees wrote in 2017 a protest letter denouncing Raoult’s dictatorship. A quote:
“Some of us are frequently belittled, mocked, humiliated, subjected to chauvinist remarks, inappropriate attitudes, violent verbal altercations, even threats from the hierarchy. One research engineer was threatened with professional death…”
The institute reacted by writing a letter to the Minister for Research announcing to punish the whistleblowers (see this blog post), whom Raoult described as “five or six grumpy jealous” and “bitter people“. This is revealing about how URMITE is run:
“A former research engineer URMITE explains that Didier Raoult works “with a table in his head” . “A cross-tabulation with two columns. He regards you more or less, depending on your status, doctor, pharmacist, researcher, engineer .. . And more or less depending on whether you are a man or a woman , he says. We had group meetings on Friday and I have often seen women from crying. “
Raoult demands results from his serfs, unconditionally:
“These tensions in the work are also felt by some doctoral students who describe situations of harassment. “Our research director, close to Didier Raoult, was struggling to handle the pressure that he put on him to get results, says one of them. Suddenly, a pyramid, the pressure fell on us.” He remembers meetings on “work in progress” where students whose work did not convince were humiliated by the research directors, with Raoult at the top.”
In March 2018, in the aftermath of the sexual abuse scandal which he tried to hush up while threatening the victims, Raoult announced:
“I thank you for having described this place as a brothel. I installed a condom machine “
Later in 2018, Raoult published an opinion piece in Le Point, where he used his authority as medical doctor and expert on sexually transmitted diseases to certify that the alleged victims of sexual harassment should not to be believed, not even by the police. In March 2020, Raoult brought back the sacked sex offender and arranged for him a job at an IHU Mediterranean spin-off. The unions wrote a protest letter, as Marsactu reported on 1 May 2020.
Now consider this. Raoult’s past papers show falsified data, which even resulted in his ban by ASM for one year, to which Raoult responded with threats of lawsuit. He is a patriarchal control freak and a misogynous bully who violently punishes all disagreement and uses threats against whistleblowers and victims to achieve compliance. He is pathologically resistant to criticism and believes to be infallible and omniscient: Raoult denied anthropogenic climate change in 2013 and before that, the microbiologist even denied evolution in his 2011 book “Beyond Darwin“. Raoult’s new study on chloroquine as the cure for COVID19 is obviously flawed, at best.
Should we really trust his claims and put our all lives in his hands?
The article was significantly updated since it first appeared.
Update 7.04.2020
On 4 April, after being alerted by my readers on Twitter and in the comment section, I tweeted about a statement by the International Society for Microbial Chemotherapy (ISAC), which issues the Journal of Antimicrobial Agents (IJAA). That was now picked up by international media an credited to Retraction Watch. The statement, signed by the society’s president Andreas Voss, was published on 3 April:
“ISAC shares the concerns regarding the above article published recently in the International Journal of Antimicrobial Agents (IJAA). The ISAC Board believes the article does not meet the Society’s expected standard, especially relating to the lack of better explanations of the inclusion criteria and the triage of patients to ensure patient safety.
Despite some suggestions online as to the reliability of the article’s peer review process, the process did adhere to the industry’s peer review rules. Given his role as Editor in Chief of this journal, Jean-Marc Rolain had no involvement in the peer review of the manuscript and has no access to information regarding its peer review. Full responsibility for the manuscript’s peer review process was delegated to an Associate Editor.
Although ISAC recognises it is important to help the scientific community by publishing new data fast, this cannot be at the cost of reducing scientific scrutiny and best practices. Both Editors in Chief of our journals (IJAA and Journal of Global Antimicrobial Resistance) are in full agreement.”
I contacted Voss and asked him if the paper will be retracted. Voss replied:
“ISAC is not the publisher. That is Elsevier and as according to them all rules and industry standards were followed a retraction is not what they consider.“
Voss then added:
“we own the title of JGAR but not of IJAA. Still, IJAA is an “official society journal” and as such we feel the responsibility, which is why we expressed our concerns.“
So it seems Elsevier put their foot down and said no.
Update 10.04.2020
ISAC now replaced and backdated the statement. As I was told by Voss, this happened on orders from Elsevier, who apparently decided ISAC scientists are not qualified to form an opinion about clinical research. The original ISAC statement from 3 April is deleted and replaced with a joint statement of ISAC together with Elsevier. The critical first paragraph is gone, but this is added:
“At present, additional independent peer review is ongoing to ascertain whether concerns about the research content of the paper have merit. Given this process of post-publication assessment is on-going, it would be premature to comment at this time. The study authors have been contacted and asked to address the concerns. Depending on the nature of their response, a correction to the scientific record may be considered in accordance with the policies of Elsevier and the Committee on Publication Ethics (COPE): https://www.elsevier.com/editors/perk/corrections-to-the-record.”
Update 12.04.2020
Now both statements are online: the one from 3 April by ISAC, restored uncensored, and the joint statement from 11 April with Elsevier, as separate release. Thanks ISAC.
Read also the follow-up reporting here and here
Update 18.03.2021
I removed the previous update as it was misleading.
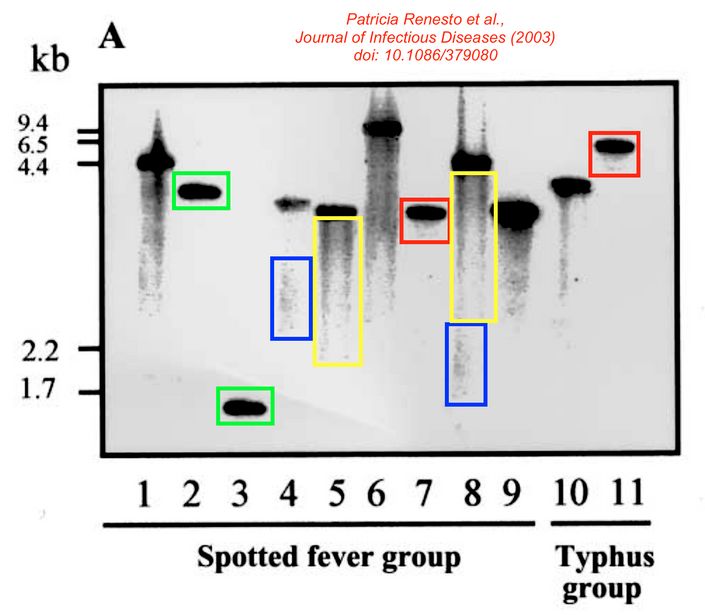
Here is something better, more data fakery by Team Raoult, spotted again by Elisabeth Bik!
Patricia Renesto, Pierre Dehoux, Edith Gouin, Lhousseine Touqui, Pascale Cossart, Didier Raoult Identification and Characterization of a Phospholipase D–Superfamily Gene in Rickettsiae The Journal of Infectious Diseases (2003) doi: 10.1086/379080
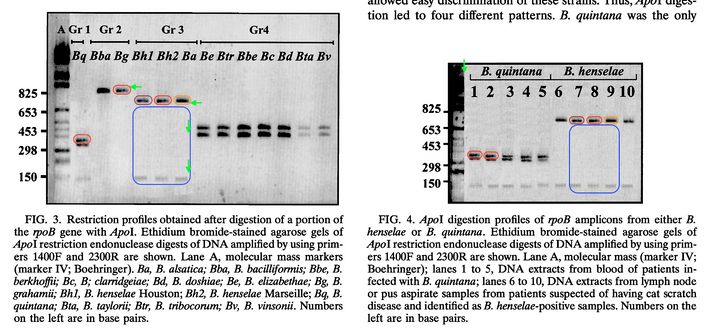
P Renesto, J Gouvernet, M Drancourt, V Roux, D Raoult Use of rpoB gene analysis for detection and identification of Bartonella species Journal of Clinical Microbiology (2001) doi: 10.1128/jcm.39.2.430-437.2001
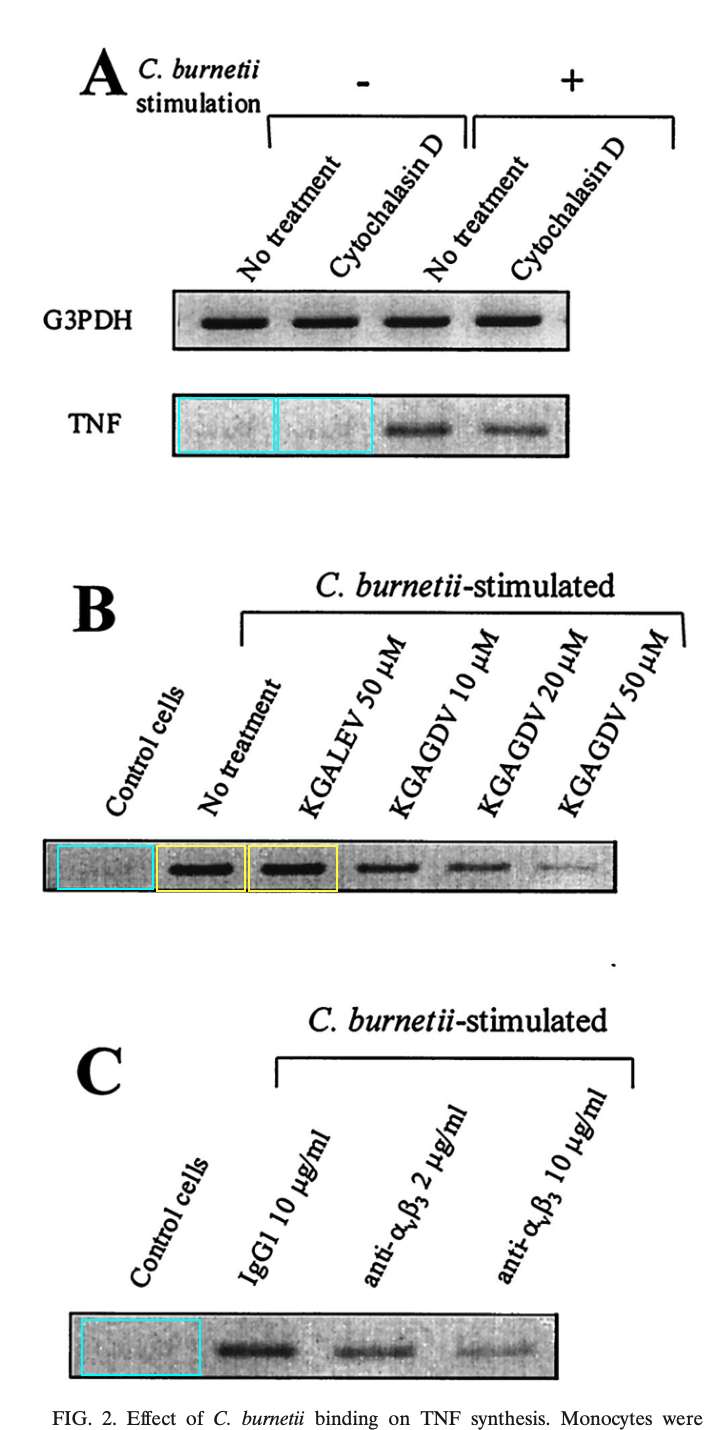
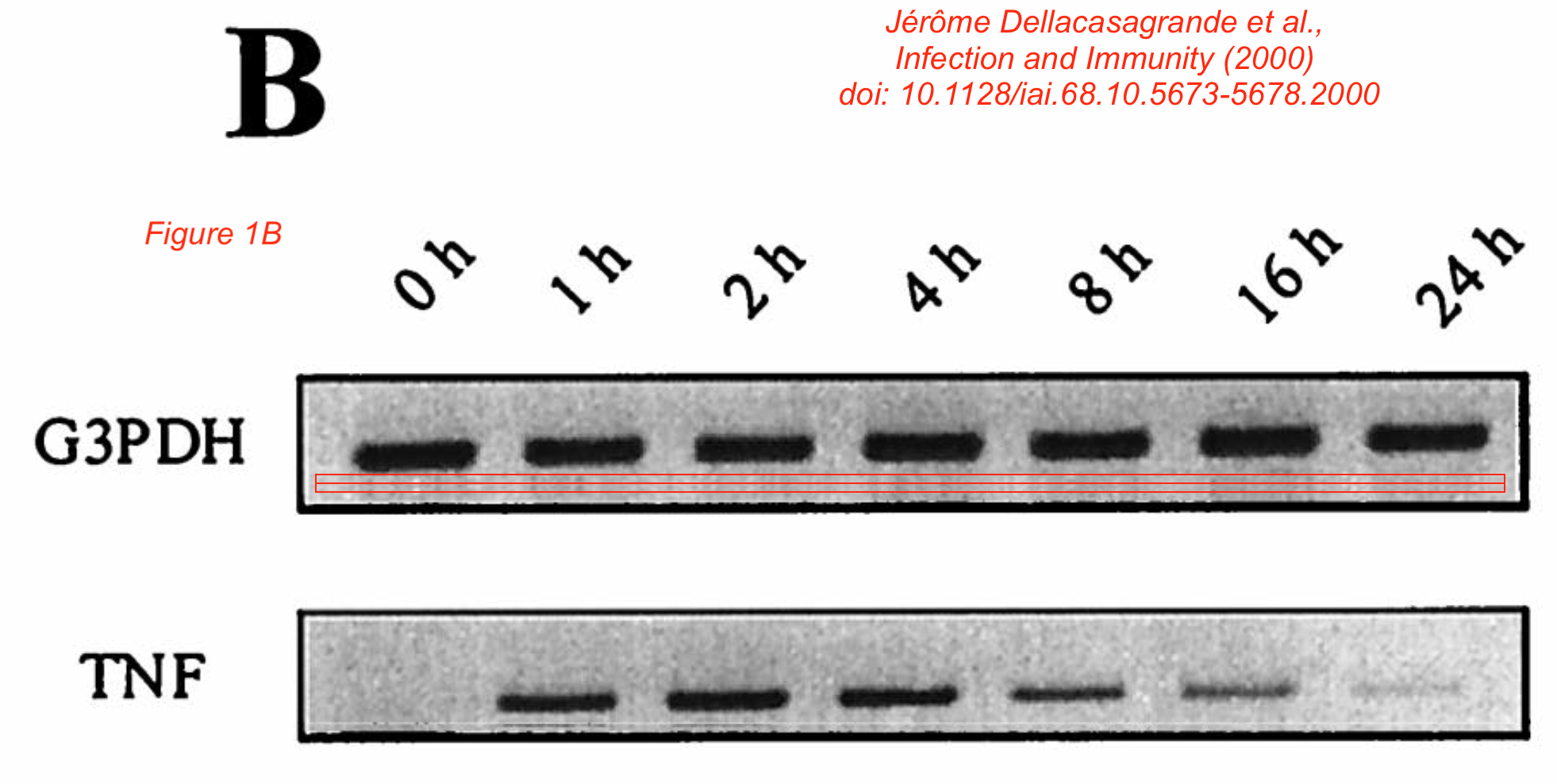
Jérôme Dellacasagrande, Eric Ghigo, Sarah Machergui-El, Hammami, Rudolf Toman, Didier Raoult, Christian Capo, Jean-Louis Mege alpha(v)beta(3) integrin and bacterial lipopolysaccharide are involved in Coxiella burnetii-stimulated production of tumor necrosis factor by human monocytes Infection and Immunity (2000) doi: 10.1128/iai.68.10.5673-5678.2000
Update 30.06.2022
The sexual harasser and racist discussed above has been finally named, by Figaro and other French media in May 2022. It’s Eric Ghigo.
He is on trial now, defended by the IHU lawyer likely paid by tax money as usual.
Donate!
If you are interested to support my work, you can leave here a small tip of $5. Or several of small tips, just increase the amount as you like (2x=€10; 5x=€25). Your generous patronage of my journalism will be most appreciated!
€5.00


{kind=link}
COVID-19: a tragedy that the humane among us will always remember, for reason of compassion.
Raoult and Trump: men we will soon forget, for no worthy reason to remember them.
LikeLike
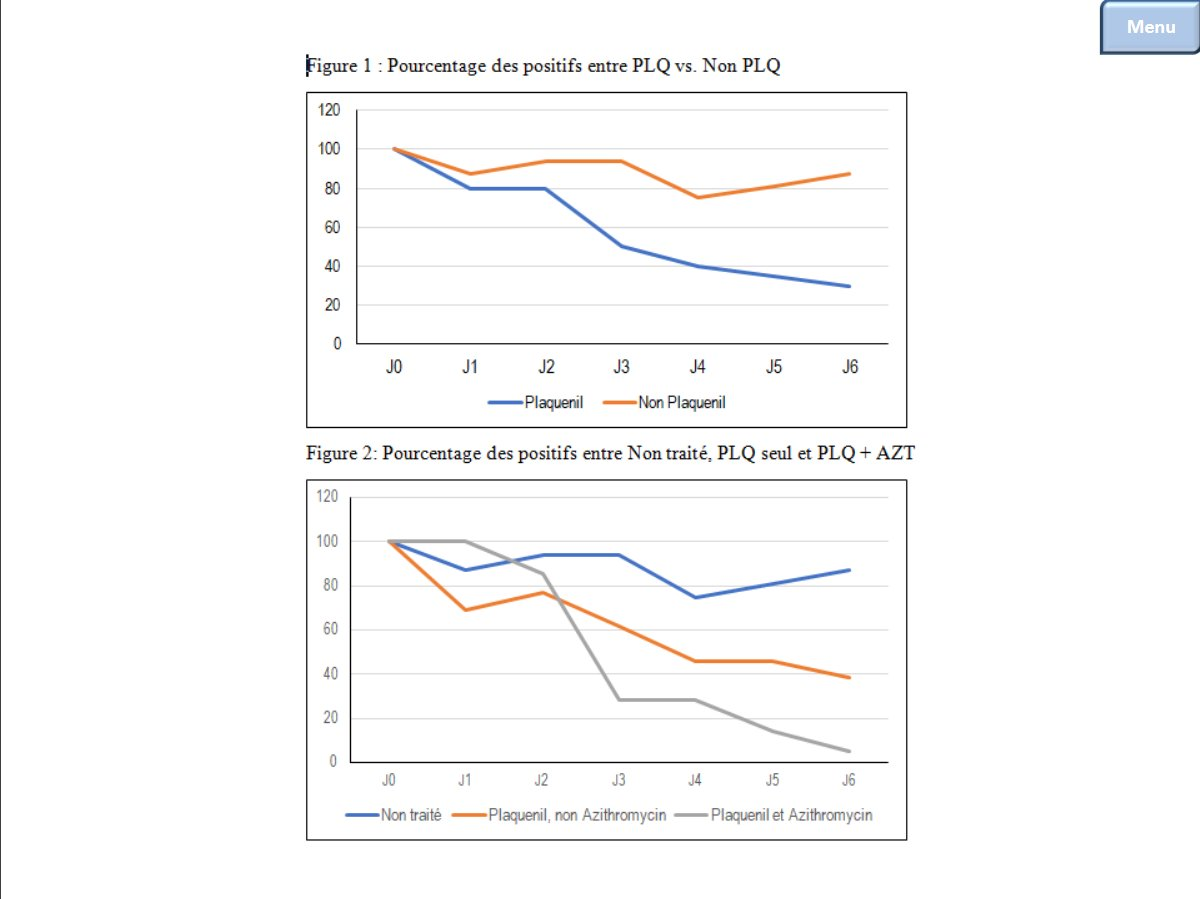
I have to say that the 80-patient cohort (https://www.mediterranee-infection.com/wp-content/uploads/2020/03/COVID-IHU-2-1.pdf) is also flawed. My analysis is here. https://twitter.com/houndcl/status/1243983427461767171.
Figure 1: percentage was calculated as [N.positives] / [N.total], instead of [N.positives] / [N.tested].
— The “N.D” = negative.
This makes a little sense, because once result is negative, doctor is unlikely to order another test.
Six patients (HCQ + AZ) from the first study were also included in this cohort, in which Patent No. 5 DID NOT have PCR data at day 1 and day 2. However, Figure 1 shows that ALL 80 patients were tested.
— This time, “N.D” = tested, but I am happy that Dr. eventually found the missing data! Congrats.
Suppl Table 1 shows that 2 patients, one transferred to ICU and one dead, “still have Ct < 34”. Based on this, author concluded that “The number of patients presumably contagious (with a PCR Ct value<34) steadily decreased overtime and reached ZERO on Day12 (Figure 1).”
— Yeah, “N.D.” due to patient loss does not count.
In addition to NO CONTROL design and the amazing 15% fever rate, the whole study is a crap.
LikeLiked by 1 person
LikeLiked by 1 person
I also recognized the 15% fever-free-patients. However the report says, that best results are obtained with HCQ and AZT, if there is not yet fever, which means, that the alveolar-space, i.e. alveolar-macrophages have not yet been affected, but the naso-pharyngeo-bronchial space. That makes the difference in pathology, viremia, and therapeutic planning. which has to be considered, and – correctly reported.
LikeLike
One cannot simply compare the data of chloroquinine (CQ) in vitro (cell cultures) with data of hydroxychloroquinine (HCQ) in patients with COVID-19 virus infection. Both substances have different pharmacokinetics in humans. Both substances are concentrated in the erythrocyte (leucocytes?), have a high plasma binding, and consist of racemic mixtures. HCQ has therapeutic (anti malaria) plasma concentrations between 39 ng / mL to 79 ng / mL, a much higher concentration is found in the erythrocytes (plasma-ERY-ratio=1:7), similar to CQ with a plama-ERY-ratio of 1:5 (Goodman & Gilman
s The pharmacological basis of therapeutics, 12. edition, page 1939t). Toxic concentrations of CQ in humans start at 0,25 microgram/mL corresponding to 0,5 microM (Goodman & Gilmans The pharmacological basis of therapeutics, 7. edition, page 1678).The clinical study on patients suffering from COVID-19-Virus-infection is based on preclinical results from cell cultures, infected with SARS-Corona-virus and addition of CQ. CQ was added experimentally in cell cultures up to 10 microM corresponding to 5190 microgram / liter (Martin J Vincent,1 Eric Bergeron,2 Suzanne Benjannet,2 Bobbie R Erickson,1 Pierre E Rollin,1 Thomas G Ksiazek,1 Nabil G Seidah,2 and Stuart T Nichol 1
1Special Pathogens Brach, Division of Viral and Rickettsial Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia 1600 Clifton Road, 30333 USA
2Laboratory of Biochemical Neuroendocrinology, Clinical Research Institute of Montreal, Montreal, 110 Pine Ave West, QCH2W1R7 Canada;
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Virol J. 2005; 2: 69. Published online 2005 Aug 22. doi: 10.1186/1743-422X-2-69).
This in vitro reported COVID-19-virus-elimination concentration range, i.e. 0,1 micro molar to 10 microMolar, would be considered as being toxic in humans, according to Godman & Gilman, 7. edition.
Free proportions of HCQ and CQ, volume of distribution and racemic concentrations are not comparable. The results from the cell cultures with SARS virus and CQ are an indication, that should be followed up in vivo. The researchers should have analyzed the blood of their COVID-19-patients for the pharmacokinetics of racemic compounds of HCQ in plasma / erythrocytes / leucocytes. Lacking that information, it is very premature from a medical point of view to draw therapeutic end results for the medical treatment of COVID-19 patients with HCQ, as reported by Professor D Raoult (didier.raoult@gmail.com) from IHU Mediterranee Infection, Marceille, France, 2020, publishes under “Clinical and microbiological effect of a combination of hydroxychloroquinine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: an observational study”.
On the other hand, one could regard this observational study as an important step further for elucidation a ratio of therapy of COVID-19.
LikeLike
The first to publish about the effectiveness of chloroquine against SARS coronavirus was the American Centers For Disease Control (CDC) during 2005 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1232869/
Then the Chinese confirmed that on their official TV
LikeLike
Can you read beyond the heading? Do you know the difference between yourself and a dish of a cell culture monolayer?
https://dx.doi.org/10.1186%2F1743-422X-2-69
LikeLiked by 2 people
Lol. For someone who asks the Question “BUT WHAT IF RAOULT IS RIGHT AND IT WORKS?????” you go on with a stream of personal attacks and do not address your own question.
Much in here is written to not even hide the BIAS dripping from it as if you wrote it in a fever pitch of Hate.
Nobody who reads this comes away feeling like you have even been close to…”Objective”..
LikeLike
Gary, he adds “I hear you ask” to that. I.e. it’s not a question he is asking, but rather one that he has heard asked.
LikeLike
But it doesn’t work. That’s the point.
LikeLiked by 1 person
One cannot simply compare the data of chloroquinine (CQ) in vitro (cell cultures) with data of hydroxychloroquinine (HCQ) in patients with COVID-19 virus infection. Both substances have different pharmacokinetics in humans. Both substances are concentrated in the erythrocyte (leucocytes?), have a high plasma binding, and consist of racemic mixtures. HCQ has therapeutic (anti malaria) plasma concentrations between 39 ng / mL to 79 ng / mL, a much higher concentration is found in the erythrocytes (plasma-ERY-ratio=1:7), similar to CQ with a plama-ERY-ratio of 1:5 (Goodman & Gilman
s The pharmacological basis of therapeutics, 12. edition, page 1939t). Toxic concentrations of CQ in humans start at 0,25 microgram/mL corresponding to 0,5 microM (Goodman & Gilmans The pharmacological basis of therapeutics, 7. edition, page 1678).The clinical study on patients suffering from COVID-19-Virus-infection is based on preclinical results from cell cultures, infected with SARS-Corona-virus and addition of CQ. CQ was added experimentally in cell cultures up to 10 microM corresponding to 5190 microgram / liter (Martin J Vincent,1 Eric Bergeron,2 Suzanne Benjannet,2 Bobbie R Erickson,1 Pierre E Rollin,1 Thomas G Ksiazek,1 Nabil G Seidah,2 and Stuart T Nichol 1
1Special Pathogens Brach, Division of Viral and Rickettsial Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia 1600 Clifton Road, 30333 USA
2Laboratory of Biochemical Neuroendocrinology, Clinical Research Institute of Montreal, Montreal, 110 Pine Ave West, QCH2W1R7 Canada;
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Virol J. 2005; 2: 69. Published online 2005 Aug 22. doi: 10.1186/1743-422X-2-69).
This range of concentration would be considered as being toxic in humans, according to Godman & Gilman, 7. edition.
Free proportions of HCQ and CQ, volume of distribution and racemic concentrations are not comparable. The results from the cell cultures with SARS virus and CQ are an indication, that should be followed up in vivo. The researchers should have analyzed the blood of their COVID-19-patients for the pharmacokinetics of racemic compounds of HCQ in plasma / erythrocytes / leucocytes. Lacking that information, it is very premature from a medical point of view to draw therapeutic end results for the medical treatment of COVID-19 patients with HCQ, as reported by Professor D Raoult (didier.raoult@gmail.com) from IHU Mediterranee Infection, Marceille, France, 2020, publishes under “Clinical and microbiological effect of a combination of hydroxychloroquinine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: an observational study”.
On the other hand, one could regard this observational study as an important step further for elucidation a ratio of therapy of COVID-19.
LikeLike
Excellent article in the tradition of muck raking. Everybody should be skeptical about an alleged fraud, especially when it’s touted by fake news organizations like Fox and parroted by proven con men like Trump. Keep up the good work. The hallmark of a dying and inquitous social arrangement is the inability to agree on the simplest of facts.
LikeLike
Everybody is quick to call everybody a conman and slap a MeToo on it for good measure these days. Bu I am still undecided on the efficacy of HCQ
LikeLike
This recent article argued that the dose of hydroxychloroquine required for clinically useful anti-COVID19 efficacy is below toxic levels
https://www.nature.com/articles/s41421-020-0156-0
LikeLike
I used to work at Raoult’s lab in Marseille and I confirm the previous testimony from H-perm concerning the crazy atmosphere in this institute .
Some positive points : IHU mediterranée Infection is a very well-equipped medical reserach institute and the staff (engineers, technicians, admin managers, researchers) are individually extremely competents. Raoult tried to have the most international research center and he welcomes students from various countries.
But …
because Prof Raoult is authoritarian, technical staff from IHU dedicated to research may fear to say that something is wrong or not working. And it’s this behaviour which, for me, could be a serious barrier for research integrity in some of his scientific work.
Bullying people presenting their work during the weekly staff meeting at the Prof Raoult’s lab was quite common. People were giving a 5 min –talk about their progress. This time was never a time for discussion between Prof Raoult and the presenters : people were just showing their slides in silence, Raoult was thinking , sometimes talking to one of the other professors. You have just to answer to specific questions and not invited to give any point of view. Some engineers, especially the new ones, were trying to argue with prof Raoult but they didn’t last long in the institute.For those who tried, Raoult had also this usual reply : « You are not paid for thinking ».
When Raoult was not in a good mood, this staff meeting were like a roman circus game where people liked to see which one of their colleagues will be destroyed. The ones who did huges efforts to show nice work were preferentially targeted : Once, one of his recent co-author turned into red at the edge of crying while Raoult just denied his work in front of all the medical staff and crudely make fun of his work. I also saw two engineers crying when presenting their results until he suddenly stop their speech because they were not enought reactives to answer his questions.
His behaviour encouraged some of the technical staff of the IHU to hide negative results, or any problems concerning on-going experimentations. People used to discharge their failings to others so problems were never solved. And a simple mistake could become then a real problem. A lot of people had short-term contracts so they were hoping to get a permanent position and they were completely cared to loose their job. So they were ready to do anything to stay in the institute.
In terms of feelings, people at the IHU are either scared by Prof Raoult, either completely enthralled by him or either trying to take advanges of him and his mediatic/political influences. By the fact, some technicians and engineers are captivated by him and are mimicking him : bullying other staff especially those who have a fragile personnality.
In this context, it’s difficult to imagine how a technical staff (in charge to prove that the head of their Institute was right) will be able to report any negative results or limitations of the study during their investigations about the efficiency of combination of hydroxychloroquine/ azithromycine against covid19. Especially after the youtube video announcement posted by Raoult saying « Chloroquine will work ».
So when you know the context of the working environment at the IHU med Infection and you see that the published results have some biaises, you have to be cautious. And it’s fair to confirm any encouraging results in other institutes.
LikeLiked by 3 people
This commentary is important, as much i like Raoult and his strong personality, as much it can be a double edge knife if his student and employees are scare of him..
LikeLike
As much as you like him and his strong personality????
He acts like an authoritarian and he’s deceptive. That puts peoples lives in danger.
LikeLiked by 1 person
I request all you learned people to finally get to the gist of the article and all the comments for scientifically illiterate people like me that in your learned opinion
1 DO YOU THINK HYDROXYCHLOROQUINE TREATMENT WOULD WORK.
2. DESPITE ALL THE FAULTS CAN WE TAKE DIDIER RAOULTS CLAIM THAT COVID 19 CAN BE TREATED WITH THIS.
3 WHAT ARE THE RESULT TRENDS FROM THE FIELD WHERE THIS TREATMENT IS BEING GIVEN. IS IT SHOWING POSITIVE RESULTS IN MAJORITY CASES OR NOT.
Thanks
LikeLike
There are better alternatives which should be tried first.
LikeLike
Guys m not at all related to medical science m just a common citizen trying to find answers and positive news to further tell my kids and family. All the hublabo about hydroxychloroquine gave us hope that all this might be over someday not too far. From what I understand that one cannot accept the snail paced highly meticulous approach of developing a cure when people are dying. What I want to know is did the treatment kill the virus in a lab. If it did then was it tried on patients, what was most of the outcome which side is the scale tilting. Then is it being used as a treatment at a larger scale? If yes then what do the results indicate is it working on most of the patients or not. Why to complicate it so much. There are around half a million people infected so no death of subjects. If I was to get ill tomorrow I would want a treatment to be given to me which was working in most of the people. As long as it works I dont care about any statistics and if it doesn’t work on me then try the second option like Remdesivir or something.
Also if roult is wrong what about anecdotal success stories coming across the world like that in india.
Third in india rajasthan people were cured with hydroxychloroquine or chloroquine plus kaletra (mix of HIV drugs Lopinavir/ritonavir) but in another study the HIV drug Lopinavir/ritonavir were found to be not working. Similarly a Chinese study showed hydroxychloroquine didn’t have much affect alone but then again a person was treated in india with same mix. So has someone tested that maybe they work well together so why is it not quickly tested on a few patients by giving hydroxychloroquine and Lopinavir/ritonavir and then share the results with the public.
Such fast most pandemic would require such fast moving research speed one cannot be taking thier own sweet time as if everything is normal and flowers are blooming and people are dancing.
Lastly why are the authorities not sharing the information on what is going on in the trials or what kind of results are being achieved with certain medicine as of now. So that people are well aware and also gain hope and positivity. Something that is badly needed in today’s time.
In the end I apologize if I have said anything wrong or overstepped my bounds as I am an illiterate when it comes to science.
LikeLike
Just because someone received the drug and got better does not necessarily mean that he got better BECAUSE of the drug. That’s why we need clinical studies and not anecdotes like “people were cured”. Were they cured, or did they simply get better (like most corona patients do)?
LikeLiked by 1 person
As with any pneumonia, gentle but regular exercise is important.
Breath. You are Indian, do Pranayama.
As this virus tends to lower blood pressure, I’ve seen people go to bed and stay there.
They slowly drown. Fighting the infection is important.
Finding stimulus to do so, outside os social means may difficult: you must look within.
Gentle antiviral Sambuca and Amla which also stimulates the lungs are ancient ayurvedic remedies.
They are accepted in Western medicine too. And are safe to use.
LikeLike
Pingback: Chronique des jours étranges – Les étapes du deuil | Le blog de Borée
Pingback: Hydroxychloroquine and azithromycin versus COVID-19: Grift, conspiracy theories, and another bad study by Didier Raoult – Science-Based Medicine
Some points to remember. Every SARS-COV2 infection is unique, because like other RNA viruses it mutates so fast that every codon in its genome will be changed many times in viruses within the resident population during the course of an infection. Every individual is unique in terms of their immune system, infection history, nutrition, health issues, etc., so interactions with the virus will vary considerably. And societies differ greatly in the extent to which they can mobilize effective measures to prevent viral spread and care for those who become infected. There will not be one solution to this problem, no matter how many snake oil salesmen roll into town trying to sell us one. A truly effective society would deal with these clowns in the time honored fashion, by tarring and feathering them and running them out of town on a rail. As it is, we at least have Leonid’s cartoons.
LikeLiked by 2 people
Pingback: Dider Raoult, le génie de la chloroquine qui sauvera le monde du COVID-19 » Simplement correct | Simply correct
Pingback: Call for calm amid hunger fears as Zimbabwe goes into lockdown - Concious Media Studios
Hydroxychloroquine proves ineffective against coronavirus in small Chinese trial
https://geneticliteracyproject.org/2020/03/30/hydroxychloroquine-proves-ineffective-against-coronavirus-in-small-chinese-trial/?fbclid=IwAR3HYHI-YovVv9D69cFJkDD4qayxGWrXXbGDviZYzLMOZNpKFkKIX41j8m4
LikeLike
Pingback: Chloroquin: Zu früh gefreut? Oder: Wie weit kann Euphorie gehen? – relativ fiktiv
Pingback: Sgamati! Tutto falso, ovunque! E' la libertà di stampa!!! - Far-Falla
I am an environmental microbiologist native of Marseille where I did all my university studies. I am not particularly a fan of Prof. Raoult and I looked at all you wrote with interest, particularly the extensive critics of his 1st “clinical assay” of HCQ + azithromycin treatment. As a microbiologist, there is however a little point where I believe that you did nor report the correct information.
Indeed, you wrote the following: “…and he is so important that he named two bacteria species after himself: Raoultella planticola and Rickettsia raoultii”. In modern microbiology, no one will publish the description of a new genera or new species of bacteria that he isolated by giving himself his name to the new described mircroorganism. If you take a look to the papers where Raoultella planticola and Rickettsia raoultii have been described, you will see that Prof Raoult was not an author of the articles:
https://www.microbiologyresearch.org/content/journal/ijsem/10.1099/00207713-51-3-925
https://www.microbiologyresearch.org/content/journal/ijsem/10.1099/ijs.0.64952-0
Of course that some of the authors of these papers were closed collaborators of Prof. Raoult, but it is very common in bacteriology that new genera or species are named according to the name of researchers who made a great contribution to the field of microbiology and this of course is often done by past collaborators of these researchers. Below some examples of this:
Methanospirillum hungatei named in honour of Prof. Robert Hungate
Desulfomonile tiedjei named in honour of Prof. James Tiedje
Syntrophomonas wolfei named in honour of Prof Ralph Wolfe
Thermotoga lettingae named in honour of Prof. Gatze Lettinga
Garciella nitratireducens named in honour to Dr. Jean-Louis Garcia
etc, etc, etc.
Then, by writing the text as you did, it seems that you want to give the feeling that Prof. Raoult has an oversized ego. You are maybe true, but the argument that you used here is not valid. As a consequence, I believe that you should rephrase this sentence or eliminate it from your article.
LikeLiked by 1 person
Thanks for sharing this. However, the authors of both papers are based in Marseille. I will adjust the sentence acocordingly
LikeLike
Pingback: Καλά νέα: Αποτελεσματικά φάρμακα και υποσχόμενες θεραπείες για τη νόσο Covid-19 - virtual reality