
This is my review of the new book by Jill Fisher, professor for social medicine at the University of North Carolina in Chapel Hill. The book is about the phase 1 clinical trial industry, where drugs are tested on healthy volunteers for adverse effects, or as the pharma prefers it, “adverse events”, to distinguish between causation and correlation. This is why the book is titled “Adverse Events“, which I received gratis from the publisher upon my request to author, there was no other financial incentive.

Phase 1 clinical trials either test new unapproved drugs before moving to phase 2 trials on actual patients, or they test combinations or dose escalations of drugs already approved and on the market. Not always are animal tests completed before pharma industry moves into human testing on healthy volunteers, in fact the current COVID-19 pandemic is the best example how recklessly rushed medical product pipeline can be, with coronavirus vaccine candidates reaching phase 3 trials in absence of any reliable laboratory or preclinical data, and despite utter absence of any past clinical successes of same technology.
Adverse events are not just a risk at phase 1 trials, they are actually the very purpose. Pharma sponsors want to see exactly which kind of adverse events their drugs can cause, and what the highest tolerable dose is. Every participant must be prepared to suffer nausea, headaches, diarrhoea, rashes, changes in heart, liver and kidney function, even hallucinations, nightmares or sleep paralysis. The idea, accepted by all sides, the participants, the investigators and the sponsors, is that those adverse effects are acceptable because they are temporary and resolve quickly. This is why, all considered, phase 1 trials are usually relatively safe, which leads some academic elitists ethicists to dismiss all ethics concerns and even to claim clinical trials would offer a safer job for working class proles than blue collar professions. This despite a rate of 1-4% of severe adverse effects, with people ending up in emergency care, or even dead. Such attitude, as aside, might explain the recent call for human challenge trials with the coronavirus.
The book is not about the machinations of the pharma industry, or about the process of drug discovery. It is an observational and interview-based field study of the demographics and socio-economic reality of the so-called “healthy volunteers” who participate in phase 1 clinical trials. And the demographic reality, at least in the United States of America, is not what we are expected to believe, even by academic experts.
Black and White
While writing this book review, I did a Google image search for “healthy volunteers in phase 1 clinical trials”. The news articles and press releases I found (all from the US) showed White participants, often female. The reality, which Fisher presents, is however exactly the opposite.

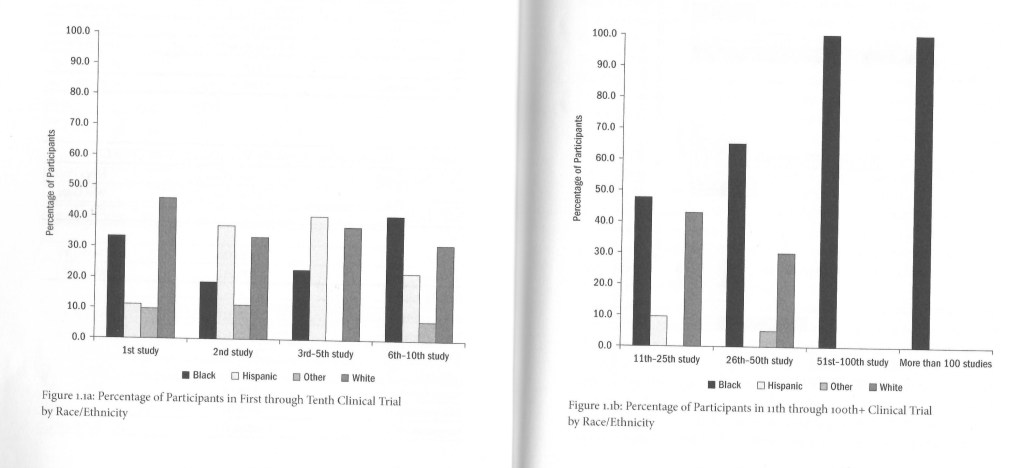
Fisher offers a model of “imbricated stigma”, where various social disadvantages overlap the lives of healthy volunteers like roof titles, driving them to chose the career of a lab rat or a human Guinea pig. Their bigger worry are not some possible transient adverse events in clinical trials, but the real and permanent adverse life events they deal with daily, as Fisher puts it. Race, poverty or sudden financial needs, incarceration history (which in US is equivalent with unemployment), being an undocumented or even a legal immigrant, or a sexual minority, personal and family troubles, all these form an imbricated stigma which leads these people to chose phase 1 clinical trials as their (sometimes only) source of income. At the end, Black, LatinX and Native Americans are extremely overrepresented among trial participants. Because this is America.
Thriving Industry
Fisher interviewed trial participants in 6 clinics: two on the East Coast, two in the Midwest and two on the West Coast. One was a small academic site (but servicing pharma industry), 4 were commercial contract organisation (2 large and internationally operating, 2 small and local). One should be aware that Fisher saw the better sites, since the really bad ones simple never replied to her or didn’t let her in.
Research for this book took place between 2009 and 2010 and started with an East Coast trial site of a pharma giant, run very smoothly and professionally. This kind of sites were already rare back then, because of the costs and in particular because of the responsibility pharma industry shoulders when doing the trials itself. In fact, the most participant-friendly and the most responsible trial sites are those operated by Big Pharma. Academic sites are technologically less advanced, and the worst sites are small commercial trial operators to whom Big Pharma outsources the job. To these “contract research organizations” (CRO), it is the pharma industry who is the valued customer whom they need to make happy, definitely not the human volunteers, who are treated accordingly.
The CRO sites are often located dangerously far from hospitals, on the assumption that nothing will go wrong, or if it will, the staff will take care of it. To further increase the profits, costs are cut by reducing participants’ compensation (including via inappropriate fines), coercing participants into additional procedures unpaid, hiring inexperienced staff, as well as simply providing little comfort and low quality food. One CRO offered not enough chairs to sit on, with another they were broken, yet another even made participants sign an informed consent that the food tasted nasty. At one small CRO, the food was better, but nurses, phlebotomists and kitchen staff were the same people. In reverse, participants judge by the way they were treated and housed to build a reference for their own safety in such clinical studies, in worst cases never to return and to warn others by word of mouth. One such rundown and unsafe New Jersey clinic was described as a “ghetto” or “almost like jail“.
The transition to such CROs started in 1980ies and grew into a gigantic industry, with multiple-ward clinics with hundreds of beds. Some were closed, for fire and safety violation, research fraud or just went bankrupt overnight with the owners buggering off with the money they owed their hundreds of participants, however
“most senior management implicated in these scandals were able to survive them by maintaining the same clinics and infrastructure but operating under a different name“
From Coast to Coast
Fisher’s first experience of a trial site demographics was telling. She arrived at the Est Coast site to a waiting room with two Black men, two Black women and two White men, sitting in pairs. Fisher’s unpeerviewed observations contradict however the peer reviewed academic expert opinion. She writes:
“Because the extant literature emphasizes or assumes that healthy volunteers are young and white, it has fallen short of an accurate description of East Coast participants. In fact, the majority are black men in their thirties who are experienced healthy volunteers“.
The situation has historical reasons, since clinical trial industry used to be more established in the North-east, incidentally with a ready supply of impoverished Black trial participants. This history is also why healthy volunteers on the East Coast are more experienced and much more critical towards the pharma industry and the capitalism in general, while their more “naive” counterparts at the East Coast and in particularly the Midwest relatively only started to make this experience with the clinical trial business.
Otherwise, on the West Coast the situation regarding predominance of serial participants and their social networking was somewhat similar to the East, only that the majority of them was LatinX. Which may be due to the fact that
“Unlike those in other parts of the country, West Coast clinics are more likely to allow participants who speak only Spanish to enroll in studies.”
With the Arizona Senate Bill from 2010, undocumented residents became unemployable. Other states followed, and now there is the openly aggressive and dehumanising racism of Donald Trump regime, which has no qualms with putting LatinX children in cages and committing other atrocities on Latin Americans. Already during Fisher’s studies, US racism manifested “with non-Hispanic participants accusing Spanish-speaking immigrants of stealing study opportunities from “Americans”“.
To which LatinX participants, male and female retorted that the “anglos” can work, but don’t want to, while they, the illegal immigrants, “we don’t have another option left“.
However, in the Midwest, there were indeed more white participants, almost all of them participating for the first time, as a temporary source of income, with the “explicit connection” to the 2008 economic recession. In fact, these Midwestern first-time participants were really peculiar: they called themselves veterans of studies, having previously serially participated in marketing research of consumer products like breakfast cereals, hot chocolate and skin care products, without distinguishing between that and entering their first clinical trial to test medical drugs. Unlike the East Coast participants, the Midwesterners “made no critique of the pharmaceutical industry or capitalism“. Fisher sums up:
“Midwestern healthy volunteers are less likely to become the model organism upon which the Phase I industry relies for its data.“
The current depression caused by Trump’s disastrous handling of COVID-19 pandemic is bound to turn more white participants to clinical trials. Where they will meet even more jobless and desperate Blacks as well as persecuted and deportation-threatened Latinos, what a gold-digging rush for phase 1 trial industry this pandemic is.
Fisher tells of a Native American with an incarceration history who had two choices to avoid defaulting on his parole fees (yes, parole fees, this is America) and going back to prison: either returning to crime, or participation in clinical trials. He and another unemployable trial participant with a prison record (a Black man) felt it was their only option to earn an honest living and to stay out of jail, with a benefit of serving medical science.
The infrastructure is well in place:
“Study recruiters set up booths at job fairs and develop targeted recruitment campaigns for people of color […]. Some clinics also actively recruit immigrants, especially those who speak Spanish […] Moreover, the clinics neither confirm participants’ legal status nor do they run background checks“.
Basically, despite their advertisements with pictures of young White women, the trial sites specifically exploit the American racism to recruit their model organisms, from among the poor of Black and LatinX men who cannot find other jobs, for example due to a prison record or an illegality status.

Model Organisms
Unlike pharma industry wants us to believe, a healthy volunteer is not the same as a healthy person. Fisher explains that what trial participants really are, is model organisms for clinical research. It is not enough to be a non-smoker without traces of alcohol or other legal or illicit drugs and medicines. The prospective participants need to show specific values in a varyingly (!) defined range, be it blood pressure, liver values, lung volume, etc. Women of childbearing age are often excluded outright for safety reasons, which is why so many trial participants are male.
Thus, the healthy volunteers need to work on themselves to become the model organisms pharma industry needs. They use their own social networks to inform themselves and their colleagues about upcoming clinical trials and their requirement, which they then serially participate in, like professional freelancers. The healthy volunteers, at least the experienced ones, are certainly not naive. Lacking all expert knowledge and higher education, they are nevertheless quite able to discern and judge the risks and to ask savvy questions during the information and consent meeting before recruitment. You are only really in when you took your first dose.
Many define exactly which studies they would never enrol in. All trials warn of a hypothetical death risk, but while it scares the staff, this is not the clue what volunteers are on the lookout for. They build on their own and their colleagues’ past experience with similar drugs, judge the dose as a safety indicator, correlate the financial reward to implicated risk (even if officially trial sites are not allowed to pay based on risk, they find other ways to raise the reward to account for “inconvenience”). Many serial volunteers avoid HIV studies due to severe adverse effects, but also due to urban legends of others having contracted AIDS this way (which seems completely unfounded, unless maybe in my view, they are testing a vaccine?). At the same time, the volunteers trust in their own health (which serial participants cultivate as their most prized possession), the responsibility of the investigators, and especially the institutional review boards (IRB), to which they even occasionally complain, for example to report incompetent phlebotomy staff.
Once the human model organisms prove themselves reliable to the trialists, they get recruited again and again, even up to phoning them up when a trial comes up, while promising financial rewards much higher that the reality upon arrival. As one (White) participant, who did the studies to supplement his job as a waiter, is quoted:
“When you do your first study, you’re kind of on their list. They’ll call you; they’ll let you know when they have studies“.
Preference is given to serial participants the researchers already personally know from past studies, as Fisher puts it: “this way the staff intentionally select the same healthy volunteers over and over again“. Sure, you need a month of washout period to flush out the previous drug from your body to participate in the next clinical study, but this only applies to the same trial site. There is no central register of trial participants, and one cannot really blame financially needy healthy volunteers for being dishonest when asked about their previous trial participations. After all, despite their assurance to otherwise, the staff does not care about the truth either, all they need is to tick boxes. The lies and disregard for washout periods are known by both sides, it’s an “open secret”. The staff happily looks away when their otherwise trustworthy recruits sport fresh needle marks or traces of adhesive on their skin as evidence of very recent trial participation. The attitude is: “it’s their life. They know the risks becasue we did tell them“.
For this same reason, blood pressure or even blood samples is sometimes taken several times from same participant till it fits the range defined by the trial sponsor. Or, this also happens, the staff slightly falsifies the readings to get their “regular” serial participant admitted despite overweight or hypertension.
It continues in later stages:
“when staff ignore any rule-breaking that occurs once a clinical trial is underway, they minimize the number of protocol deviations they must report to the study sponsor.“
On the other end, trial participants are reluctant to report adverse events. One reason is, they are (justifiably) afraid to be kicked out of the trial without receiving full pay. Since healthy volunteers are paid by day, with the total reward legally fixed not upon risk, but upon the mere duration of the trial and travel costs, neither side wants to see a trial aborted due to adverse events. A Latino participant was quoted:
“I’ve seen people not say anything, and they could be sick as a dog and still take the medicine.“
The staff is well aware of the situation, but they also want the trial to run smoothly till the end, the CRO does not want to disappoint their real customer, the trial sponsor. Investigators even suspect that participants would be feigning symptoms to leave the clinic early or to get the study cancelled. Those participants prone to developing adverse events like rashes simply do not get called again, as a recruiter at the academic trial site openly admitted. On the other end, pharma sponsors pressure site investigators “to revaluate the data” of reported adverse events, hinting that they won’t be contracted again if they continue listing the symptoms as drug-related.
Adverse Effects
The lack of qualified phlebotomists at many CROs was the most serious criticism among participants, but it can get worse that an banged-up blood draw (one interviewee tells of a broken caterer and gushing blood). Because CROs want to save money at all costs, they are highly disinclined to get actual doctors and hospitals involved when something goes wrong. One trial participant developed a cyst as adverse event, his complaints were dismissed for four months because the CRO refused to pay the hospital treatment.
In most trials, the investigators need participants’ blood, which is collected quite often, to measure pharmacokinetics (the rate of drug being metabolised and excreted) and pharmacodynamics (the drug’s effect on the body and its functions). But sometimes other fluids are needed, and the one which scares participants most is cerebrospinal fluid, which is collected from the spinal column to study the drug’s penetration of the blood-brain barrier. The reason most avoid such trials is not just a hypothetical risk of cock-up and permanent injury up to paralysis, but a very real adverse effect of horrible headaches due to loss of fluid pressure on the brain should even rise from your bed once. There is a troubling and revealing episode Fisher witnessed in this regard.
A Black volunteer was led to collect his cerebrospinal fluid. He was surrounded by 4 white medical staff. The expert physician was delayed, but the staff already began by inserting the needle into the spine, without telling the locally anaesthetised) participant about that. When the older White doctor arrived, he hastily threaded the catheter into the spine, and the cerebrospinal fluid of a Black man surrounded by 5 impatient White people began to drip… onto the bed, where it soaked the drape. The stuff eventually noticed the problem and supplied a vial to collect the dripping fluid. When the procedure ended, the Black man has not uttered a word yet, nobody spoke to him, it later turned out he was totally unaware of the malpractice which happened literally behind his back. Did anyone of these 5 White people even notice they were experimenting on a human being? Did they perchance felt like dealing with a lab animal? Their next sample provider was a Latino, both participants later declare never to do a spinal tap again.
Sometimes, it is the pharma industry trial sponsor who is the problem. Many phase 1 trials are about dose escalation, where the pharma sponsors intentionally cause adverse effects in test subjects to tests the highest tolerable dose, hoping it will not cause long-lasting or even permanent damage. At one trial, participants were warned in advance that they should “plan on puking“. But at one CRO, a participant ended up at intensive care because the trial sponsor wanted to escalate the drug dose while knowing that two monkey have died after receiving a high dose of that drug. In this regard, it is worth mentioning that phase 1 human trials often commence before any toxicity or reproductive teratology results from non-human experiments are obtained.
There is an interesting attitude towards trial participants displayed by the staff. First of all, they deem all trials as perfectly safe while not hiding their low opinion of those who risk their health to engage in these. The staff always makes clear that neither they themselves nor their family of friends would ever participate as healthy volunteers, while at the same time
“staff are more likely to perceive the participants as sources of risk to the protocol rather than as subjects who are exposed to risk“.
Safe Drugs?
Fisher repeatedly discusses the implication of human model organisms phase 1 pharma industry has created. They represent namely nobody at all, not even healthy humans. Starting with the exclusion of women of childbearing age during phase 1 trials, with the results that approved drugs get recalled from the market having proven toxic to female patients. The phase 1 participants are indeed mostly male and, instead of being just healthy, they are selected on case-by-case basis to fit certain safety criteria. For example, if the drug is known to lower blood pressure or heart rate, even experienced healthy volunteers will get rejected if their otherwise perfect heart is running not in the approved higher range (since the trial sponsors want to avoid adverse events). If a drug is known as somewhat toxic, certain liver and kidney values are need to buttress its toxicity. All this has little to do with actual patients expected to take these drugs after they were declared as safe in phase 1 trials. Fisher writes:
“Rather than answering the general question “How safe are these pharmaceuticals?”, Phase I trials instead tackle the narrower question “How much of an investigational drug can be given to healthy volunteers without inflicting too much harm?”“
Fisher also speculates that the “reusable” model organisms whom phase 1 trial industry repeatedly recruits might be in a way resistant to adverse effects, because only those who don’t experience bad adverse effects (or as interviews reveal, rather just don’t perceive them as bad) will be motivated to enrol in more clinical trials, serially. As opposed to that, those who complain of nausea or headache too much are seen as troublemakers and are unlikely to be admitted by the recruiters again. With all sides (volunteers, trial investigators and pharma sponsors) breaking the rules to suppress adverse events, and nobody from outside overseeing the process, how reliable is the safety profile of FDA approved drugs then? This is why adverse effects often manifest only in patients, after the drug is used nationwide.
There are many other scientific, social and demographic aspects the book addresses, which I why I do recommend that you read it. Especially during the COVID-19 pandemic, its message is very important.
The payment and the risks which the participants are expected to accept, depend on the current economical climate. The US capitalism, which is based on extreme financial and social inequality and institutionalised racism, has always provided a steady stream of desperate and competing human volunteers for phase 1 research. Fisher discusses this, and concludes:
“there is a symbiotic relationship between the Phase I clinical trial industry and the profound economic insecurity in the United States“.
Now imagine what happens now, due to Trump and his disastrous handling of the COVID-19 pandemic and the catastrophic poverty and unemployment it caused.
Disclaimer: as always, I am not paid for this review, but I did receive the book gratis from the publisher
Donate!
If you are interested to support my work, you can leave here a small tip of $5. Or several of small tips, just increase the amount as you like (2x=€10; 5x=€25). Your generous patronage of my journalism will prevent adverse events in science and medicine!
€5.00


Thank you for writing a review of what appears to be a very important book. As with these Phase 1 trial participants, I wonder if volunteers who donate bone marrow are also economically disadvantaged? The company AllCells pays donors $500 for having marrow aspirate from both hip bones, and then sells it on for $48,000 as a GMP-grade product to companies who want to use it for manufacturing cell therapy products. Another company I spoke to that is selling GMP-grade bone marrow told me they could go back to the same donor up to 3 times in a 12 month period. In Europe, donors give their bone marrow altruistically to help patients with conditions such as leukaemia. In many cases now, the haematopoietic stem cells can be mobilised with GCSF and collected from the donor’s peripheral blood so that aspiration of bone marrow is not needed. Imagine how desperate for $ you must be to subject yourself to a bone marrow aspiration 3x in one year for the purpose of helping a US company make large profits.
LikeLike
Pingback: Whom to sacrifice for Human Challenge Trials? – For Better Science
It is a very big worry if any vaccine trial is rushed. May even in the end produce exactly the opposite of the desired effects with people being rushed to crowded hospitals and thus even worse health and economic effects.
LikeLike