
Tide is turning for the media-savvy French professor Didier Raoult and his chloroquine, even US President Donald Trump is suddenly barely even mentioning the miracle drug for COVID-19. Maybe this is because the only clinical data supporting the malaria drug chloroquine cure against coronavirus comes from Raoult himself. And only after Raoult denounced controls and other basics of clinical research as unethical. Outside of Raoult’s alternative reality, clinical data from France, Sweden, Brazil and USA already now shows that chloroquine not only does not work against COVID-19, it seems to even kill. Predictably so, since the drug’s side effects are well known.
This is why chloroquine proponents changed their stance and now scream that it is wrong to treat very sick COVID-19 patients with chloroquine. Instead, they insist that the drug must be given very early during infection or even prophylactically, i.e., to healthy and asymptomatic people only. Given the evidence that the coronavirus is apparently lethal for less than 1% of the infected, you can see where this is going. The safest way to successfully heal with witchdoctor magic is to treat those who are not really ill and recover anyway.
But now Raoult seems to have gone completely off the rails. He namely attacked the data integrity expert Elisabeth Bik, on Twitter and in full Trump manner:
Heal the healthy, avoid the sick
The microbiologist Raoult is director of the Institut hospitalo-universitaire en maladies infectieuses de Marseille (IHU Méditerranée Infection) and its URMITE department, which was previously funded by the French research networks CNRS and INSERM. Both withdrew in 2018, after Raoult proved a despotic tyrant who allowed sexual harassment, discrimination and bullying to happen in his institute (read more here). There is also a history of data manipulation, for which Raoult himself was made responsible in 2006. Bik found even more irregularities in his papers, which makes sense: a bullying and totalitarian research environment with a personality cult, where compliance and fear rule, can only produce unreliable or falsified research.
Like these copy-pasted disease-spreading ticks, or these copy-pasted fraud-spreading gel bands, newly discovered at IHU:
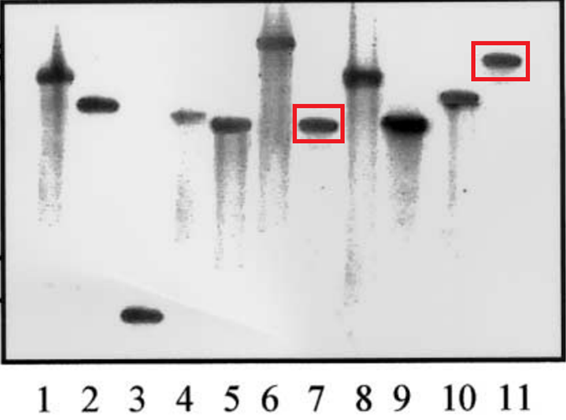
P Renesto, P Dehoux, E Gouin, L Touqui, P Cossart, D Raoult Identification and Characterization of a Phospholipase D–Superfamily Gene in Rickettsiae J Infect Dis (2003) doi: 10.1086/379080 Also “lanes two and three show concerning similarities.“
To make the insolence worse, Raoult’s approach was repeatedly criticised by Bik. When Raoult claimed to have cured 80 patients of COVID-19, without a control arm in his study, Bik summed up:
- “At enrollment, 92% of the patients had a “low” score in the National Early Warning Score (NEWS), suggesting they were not very sick.
- The average time between onset of the COVID-19 symptoms and being enrolled in the study was 5 days. This suggests that the patients had already been sick for a while.
- Only 15% of the enrolled patients had a fever. Fever is one of the characteristic symptoms of COVID-19, so people with a positive PCR but no fever are probably only mildly ill, or maybe already recovering.
- Of the 12 patients who had a fever, the mean temperature was 38.6C (101.5 degrees F).
- Only half of the enrolled patients had a lower respiratory tract infection.
- 15% of these patients required oxygen.
- Four patients were asymptomatic.“
Obviously it is easy to cure patients who are not really that sick in the first place. But what about the treatment itself? Problem is, that especially the combination of the immunosuppressive hydroxychloroquine and the antibiotic azithromycine, as promoted by Raoult, has very serious side effects which can lead to death. It should be noted that while Raoult’s IHU hospital in Marseille boasts a very low COVID-19 mortality rate of 1.7% (while refusing to treat the very ill) it is still higher than the estimate for the rest of France which is 0.53% according to this study from Institut Pasteur.
Because of Raoult, chloroquine became standard COVID-19 therapy in many countries worldwide. Including in France. Yet an observational study on 11 patients from Paris (Molina et al 2020) reported already on 30 March “no evidence of rapid antiviral clearance or clinical benefit”:
“At the time of treatment initiation, 10/11 had fever and received nasal oxygen therapy. Within 5 days, one patient died, two were transferred to the ICU. In one patient, hydroxychloroquine and azithromycin were discontinued after 4 days because of a prolongation of the QT interval from 405 ms before treatment to 460 and 470 ms under the combination. Mean through blood concentration of hydroxychloroquine was 678 ng/mL (range: 381–891) at days 3–7 after treatment initiation.
Repeated nasopharyngeal swabs in 10 patients (not done in the patient who died) using a qualitative PCR assay (nucleic acid extraction using Nuclisens Easy Mag®, Biomerieux and amplification with RealStar SARS CoV-2®, Altona), were still positive for SARS-CoV2 RNA in 8/10 patients (80%, 95% confidence interval: 49–94) at days 5 to 6 after treatment initiation.“
Sweden, which initially followed Raoult’s teachings and started to treat COVID-19 patients with chloroquine, swiftly aborted the method when patients developed severe side effects. A retrospective study on 84 patients receiving hydroxychloroquine and azithromycine from New York University (Chorin et al medRxiv 2020) also demonstrated how serious those side effects in COVID-19 patients can be:
“We report the change in the QT interval in 84 adult patients with SARS-CoV-2 infection treated with Hydroxychloroquine/Azithromycin combination. QTc prolonged maximally from baseline between days 3 and 4. in 30% of patients QTc increased by greater than 40ms. In 11% of patients QTc increased to >500 ms, representing high risk group for arrhythmia. The development of acute renal failure but not baseline QTc was a strong predictor of extreme QTc prolongation.”
That study, and a mysterious manuscript from Detroit submitted to NEJM, are discussed by Derek Lowe here.
Above the law?
As it happened, Raoult’s most recent (literally) uncontrolled clinical trials were ethically approved by his own submissive IHU. He even treated 14 year old children with chloroquine as part of his 1000 patients trial (Table 1 here, recruitment age was >12 years old), which is actually quite illegal. In his paper Gautret et al TMID 2020 Raoult admitted that his thousands of patients were kept in the dark about the risks, since none of them received a patient information sheet and an informed consent to sign:
“There is no formal consent to sign in our institution by patients“
IHU’s human guinea pigs were unaware of the experimental nature of the therapy, quite the opposite: because Raoult decreed that the hydroxychloroquine+azithromycine method must work, he retrospectively defined it a “standard treatment“. They believed to be undergoing an established, internationally approved therapy for COVID-19. Even more schizophrenically: all studies which Raoult designed in advance, with the explicit purpose to prove his therapy, were declared “retrospective” to deny the need for an ethics approval. This horrendous ethics breach passed peer review at Elsevier with flying colours. In 1 day.
On 20 April 2020, news came of Raoult being in serious legal trouble with the French authorities because of his human experiments with chloroquine:
“The National Agency for the Safety of Medicines and Health Products (ANSM), which did not authorize the second study on hydroxychloroquine (Plaquenil *, Sanofi) conducted at the institute hospital-university (IHU) in Marseille by Pr Didier Raoult, awaits that the investigators bring objective elements to demonstrate its observational nature, indicated Dominique Martin in an interview with APMnews.”
That was sure something unexpected for Raoult, after the President of France, Emmanuel Macron, has visited his lab just days before and described Raoult as “great scientist”. On 24 April IHU retorted that the study never needed any ethics approval or patient consent, because it was “retrospective”, a hair-raising argument their Italian colleagues routinely used to cover up intentional patient abuse. And anyway, Raoult and his colleagues “deemed it ethically unacceptable to conduct a therapeutic trial“.
Meanwhile, in USA, an NIH Expert Panel, convened by the National Institute of Allergy and Infectious Diseases (directed by US epidemics expert Anthony Fauci), recommended in its COVID-19 guidelines on 21 April 2020:
“Except in the context of a clinical trial, the COVID-19 Treatment Guidelines Panel (the Panel) recommends against the use of the following drugs for the treatment of COVID-19:
– The combination of hydroxychloroquine plus azithromycin (AIII) because of the potential for toxicities.”
Chloroquine is about to become a major embarrassment for everyone. And Raoult is the central figure in this international Il pleut de la merde.
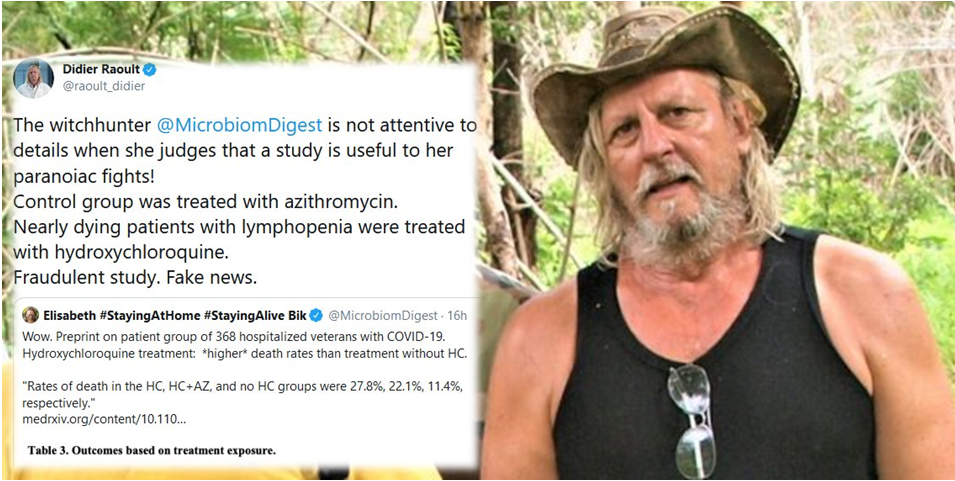
No wonder that the grand old man, unused to being contradicted or ridiculed, is losing it. The object of Raoult’s public wrath is now Bik whom he describes as “witchhunter”, as well as this study from Veterans Affair hospitals in USA:
Joseph Magagnoli, Siddharth Narendran, Felipe Pereira, Tammy Cummings, James W Hardin, S Scott Sutton, Jayakrishna Ambati Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19 doi: 10.1101/2020.04.16.20065920
The retrospective controlled clinical study found out that hydroxychloroquine-treated patients had a high risk of death and concluded:
“In this study, we found no evidence that use of hydroxychloroquine, either with or without azithromycin, reduced the risk of mechanical ventilation in patients hospitalized with Covid-19. An association of increased overall mortality was identified in patients treated with hydroxychloroquine alone.”
The study made all the big news, maybe because it was the first one from the US. Raoult (or maybe his personal assistant in charge of social media) tweeted his views:
“The witchhunter @MicrobiomDigest is not attentive to details when she judges that a study is useful to her paranoiac fights!
Control group was treated with azithromycin.
Nearly dying patients with lymphopenia were treated with hydroxychloroquine.
Fraudulent study. Fake news“
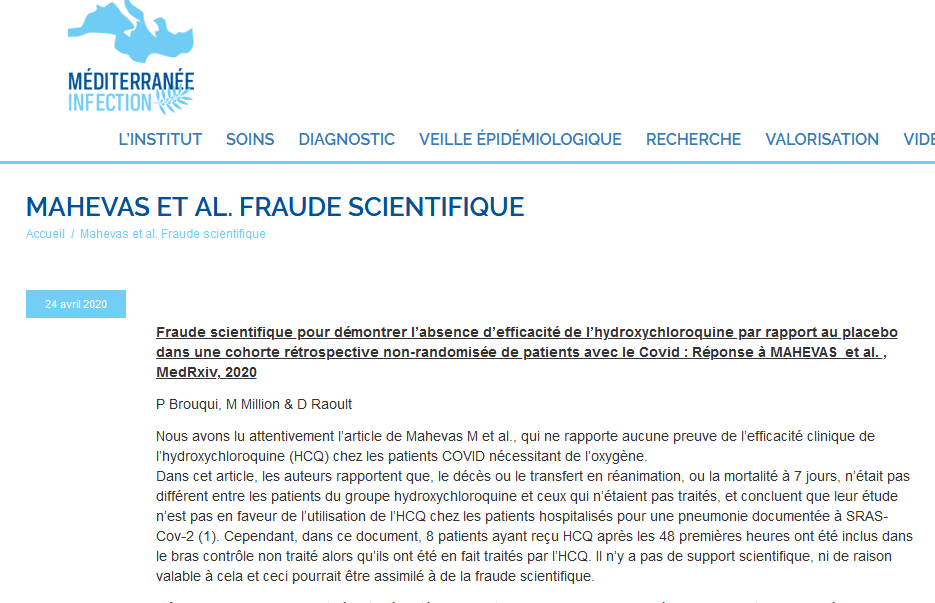
When you spend so much time admiring Trump, you start sounding like your idol. After dealing with Bik, Raoult tweeted his criticism about a study by his French colleagues in Paris and their study Mahevas et al medRxiv 2020.
Unlike his own clinical trials, Mahevas et al was really an observational study of 181 French COVID-19 patients treated after Raoult’s method, but with a control group. The paper, published on 14 April, concludes against the use of hydroxychloroquine on COVID-19 hypoxic pneumonia patients and mentions:
“Eight patients receiving HCQ (9.5%) experienced electrocardiogram modifications requiring HCQ discontinuation.“
On 24 April Raoult and his IHU issued another press release or a white paper, where they openly accused their Paris colleagues Mahevas et al of “scientific fraud“, already in the headline. Raoult’s J’accuse partners are IHU group leader Philippe Broiqui and clinic head Matthieu Million. If you naively think such institutional fraud accusations happen in the scientific community at least occasionally: not really. IHU seems to have evolved under Raoult’s leadership into a lunatic asylum for the criminally insane.
Prior to that outpour, Raoult endorsed a bizarre telemedicine (sic!) study by a Brazilian insurance (sic!), which was never published anywhere, not even as preprint. It is only available as document on the file sharing platform Dropbox (sic!):
Bik blogged about that Brazilian “study”, where 636 patients, distance-assessed by telemedicine only, themselves decided which drug to take after they self-diagnosed themselves with COVID-19 (sic!). Afterwards, the study’s authors somehow pulled up the numbers of who died and who went to intensive care, and fabricated p-values which did not fit. Bik then provided an update on 20 April:
“It was announced today that the study described below has been suspended because of ethical violations. As pointed out by Natalia Pasternak and Carlos Orsi and Ricardo Parolin Schnekenberg […], the study had already started before the ethical approval had been obtained. This could be figured out by looking at the disclosed study days in the preprint and the trial registration at the Clinical Trials website.“
But for Raoult, that was a proper scientific clinical trial. Not the one done by his US peers in the Veterans Affairs hospitals, that was a “fraudulent” and “fake news”. What about this other Brazilian study, Silva Borba et al medRxiv 2020, published on 16 April?
“The high dose CQ arm presented more QTc>500ms (25%), and a trend toward higher lethality (17%) than the lower dosage. Fatality rate was 13.5% (95%CI=6.9-23.0%), overlapping with the CI of historical data from similar patients not using CQ (95%CI=14.5-19.2%). In 14 patients with paired samples, respiratory secretion at day 4 was negative in only one patient.”
In this double-blinded phase IIb clinical trial, all patients were treated just as Raoult says, with hydroxychloroquine+azithromycine only, without those evil controls Raoult hates? Chloroquine was applied in two different doses, and the doctors had to halt the high dose arm because the patients were dying from heart failure. Raoult doesn’t talk about that study.
Doomsday cult
Instead, he lets his loyal bootlickers attack his critics. On 14 April 2020, Raoult’s IHU Marseille openly and publicly threatened a clinician Damien Barraud, who has been very critical of their chloroquine “studies” on Twitter and in newspaper interviews. IHU tweeted a demand for Baraud to be stripped of his medical licence and be sacked by his hospital employer in Metz, and announced lawsuits for libel:
As I reported before, the International Society for Microbial Chemotherapy (ISAC), with which Raoult published his initial chloroquine study Gautret et al IJAA 2020, distanced themselves from it, in a public statement from 4 April 2020. ISAC (and then the publisher Elsevier) insist however that the peer review process “did adhere to the industry’s peer review rules.” Which is strange, since it seems the paper was reviewed and sent back for minor revision on the same day it was submitted. The next day, the authors returned a revised version which was immediately accepted.

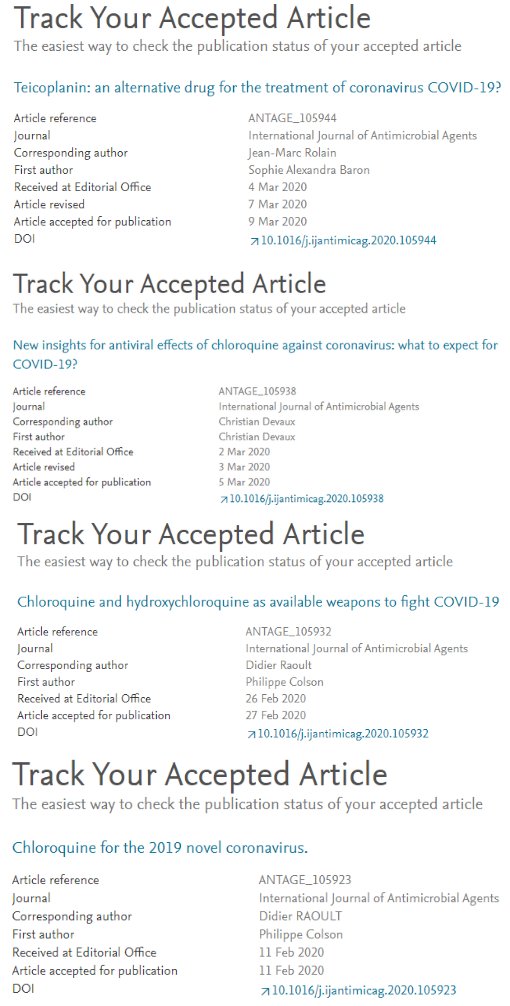
Raoult’s follow up clinical trial with 80 patients treated with chloroquine and azithromycine and without any control arm (criticised by Bik above) was published in a different Elsevier journal, and accepted the next day after submission. The first author of the new Gautret et al TMID 2020, Philippe Gautret, is incidentally associate editor of that of that journal.
Regardless of the obviously repeatedly rigged peer review process, that wretched first Gautret et al IJAA 2020 paper serves as the ONLY clinical study on which the pharma giant Novartis bases its newly announced phase 3 clinical trial in USA, on 440 patients. Do check the references here.
Not just this. Somehow Raoult’s Marseille buddy Jean-Paul Moatti managed to smuggle an opinion piece into The Lancet promoting chloroquine. The author declared no conflict of interest, despite being the husband of Raoult’s co-director at IHU, Yolande Obadia.
Now Raoult, the 1-hour-peer review man, suddenly has enough of the traditional publishing he constantly games. He tweeted his YouTube video, saying that he prefers to have his studies assessed by “confined people” at his institute than by some external reviewers he cannot control:
In that same video, Raoult is saying things which make less and less sense:
“Maybe I was capable of responding to this situation because I’m part African and part of my ancestry leave me with the idea that we should treat infectious diseases“
The signs that Raoult might be losing his mind are already there. Problem is, having cemented his totalitarian power at IHU, having stifled all dissent years ago and having surrounded himself by loyal yes-sayers only, there is nobody to tell Raoult that he is making an utter arse of himself, in public and even on video.
In that recent preprint, where Raoult claimed to have cured with chloroquine over 1000 patients mildly or barely suffering from COVID-19 (including children), he counted 5 levels of evidence that his method works. The highest level of evidence is Raoult’s own Gautret et al IJAA 2020 paper, plus two studies from China which don’t even fit. Who cares, it will sure pass peer review in one of Elsevier journals Raoult controls. It is all very surreal.

The manuscript lists these key words: “SARS-CoV-2; COVID-19; hydroxychloroquine; azithromycin; ethics; Hippocratic oath“. The last two strongly suggest that there is a kind of religious mass psychosis going on at IHU. These keywords are listed because Raoult firmly believes that it is unethical NOT to treat COVID-19 patients with chloroquine, and every doctor who insists on scientific process and evidence, breaches the Hippocratic oath of not doing harm. Nobody at Marseille laughed or told Raoult to check himself in into an asylum. The entire IHU plays his game like a devout doomsday cult on hallucinogenic drugs.
The “great scientist” believes in his delirium to be actually just like a World War I general, commanding thousands of men to get out the trenches and die for the glory of France.
What next? To be updated, proper randomized controlled clinical trials on chloroquine against COVID-19 are ongoing and might soon deliver results. But Raoult is sure a tough guy who won’t go down without a fight.
This article has been updated several times since it was first published.
Update 2.05.2020
TCM as chloroquine adjuvant?
There seems to be a clear pattern how Raoult evaluates scientific studies. Those which do not fit his general world view, are all flawed or outright fraudulent. Those which seem to support his chloroquine claims are infallible and perfect.
So now Raoult endorses Traditional Chinese Medicine (TCM) as a chloroquine adjuvant. Really, he does:
The reference is to a new preprint from Tongji Hospital in Wuhan, China, Yu et al medRxiv 2020. It reports a retrospective analysis of a clinical trial with “568 critically ill patients” with mortalities of 18.8% (9/48) in hydroxychloroquine (HCQ) group and 45.8% (238/520) in no-HCQ group. Astounding, right? Only that the Wuhan authors never mention azythromycine, while Raoult so far insisted HCQ does not help critically ill COVID-19 patients at all.
Now, the preprint by the Tongji cardiologist Wang Daowen and colleagues claims all 568 patients received “baseline treatments [..] of antiviral drugs (Lopinavir and Ritonavir, Entecavir hydrate, or Ribavirin)“. 48 of these allegedly received HCQ. The ethics approval references a clinical trial with Daowen as principal investigator, which however used only one drug: Shuanghuanglian. It is a herbal TCM concoction, the trial had 4 arms with 3 different Shuanghuanglian quantity, plus control arm. A total of 400 patients (as opposed to the preprint’s 568), nobody was treated with HCQ or any other drug mentioned in the preprint.
Unless completely made-up fraud, there is only one way to explain it: For controls, Daowen et al lied about baseline treatment because serious scientists outside of China tend to laugh at TCM. Where the extra 158 patients and the HCQ group came from, is anyone’s guess, unless invented they were borrowed from different trials or hospitals. Raoult says this is good science. Maybe he will replace azythromycine with TCM now?
Update 20.05.2020
Raoult was possibly made to resign his job, he was cited to go to China already this summer. Incidentally, by leaving France and Europe, he would escape any eventual criminal charges for illegal human experimentation.
The French newspaper Entreprendre cited his letter to Robert Lafont, the CEO of this publishing house. The online article was swiftly deleted, but here is a backup. Newspapers were quick to denounce the report as fake news and a prank, Lafort himself played stupid, but I personally am not so sure (although it is likely Raoult was never offered a job in Peking). This was Raoult’s letter, translated:
“Since you have been one of the rare journalists to have exhibited exemplary behaviour during this period, I would like to take this opportunity to reserve for you the first news: my upcoming departure for China (by the end of the summer). I was indeed recruited as Professor by the Peking University (PUHSC), the most renowned medical school in the country, which happens to be very advanced in the field of virology. It became very complicated to undertake research projects in the health sector in France, the sector being plagued by partisan quarrels, sprawling bureaucracy and political correctness. “
Donate!
If you are interested to support my work, you can leave here a small tip of $5. Or several of small tips, just increase the amount as you like (2x=€10; 5x=€25). Your generous patronage of my journalism will be most appreciated!
€5.00


Great article.
Just adding for the record that despite his own exclusion criteria Pr Raoult did enroll 10 y/o children, for which there is a 3 years jail sentence + 45k euros fine.
source : https://www.mediterranee-infection.com/wp-content/uploads/2020/03/Hydroxychloroquine_final_DOI_IJAA.pdf
see page 6 for inclusion criteria : “two primary criteria: i) age >12 years;”
see page 22 for data on patients (two 10 y/o children were included in the study)
PS it doesn’t matter if they were in the “control” group or not, they were part of the study
LikeLike
It appears the author has an axe to grind here…Me? I’d just like to see a cure found. So why do I say that about the author? Well, Let’s look at Costa Rica, and their death rate. After that, let’s look at Bahrain, and Turkey. What do they have in common? Heavy use of HCQ. Turkey just spoke up on the merits of HCQ yesterday. After that, let’s consider the doctors who have used HCQ for Lupus and RA. One in Italy tweeted yesterday that only 20 patients out of 65,000 users contracted Covid in Italy. Wow! Please try to explain it away…but it sounds like a darn good prophylaxis. And while we’re at it, the author doesn’t seem to understand that chloroquine is not the same as HCQ. Bad results for Chloroquine does not mean anything about HCQ. Think Hydrogen Peroxide vs Water. Only one molecule difference, but vastly different properties.
HCQ is an antiviral. The idea is to kill the virus. You want to use it as early as possible, so it has a better chance of killing fewer bad guys to be successful. Waiting to use it until the patient is deathly ill is an exercise in futility. It doesn’t have an ability to arrest the overreactive immune response that seems to be happening with Covid. Scientists understand this, but the media is hoping readers won’t. After all, this off patent, inexpensive drug, which has been prescribed millions of times with safe outcomes, doesn’t make the medical establishment enough money. If you want a smoking gun, start with who makes money where. At a buck a pill, there’s no financial incentive for anyone to sell HCQ. Pull back the curtain, and you will find there are several doctors in the US who are saying they are successfully using HCQ to prevent hospitalizations and deaths. And it shortens the viral cycle by a lot more than 3 days (Remdesivir). The media and AMA doesn’t seem to want you to hear about it.
LikeLiked by 2 people
After 4 months of closely following the Covid-19 fight in general and HCq in particular, it appears to me that ZINC is critical to the effective use of HCQ. HCQ may have antiviral properties especially for Covid virus in the body fluids, but once the virus gets into cells where it reproduces, then it seems the ionophore properties of HCQ are the essential component which allows Zinc to enter cells and stop the virus from reproducing there. To the extent that HCQ has some utility in fighting Covid, especially in the early phases, it may be that the patients have enough Zinc reserves for HCQ and Zinc to work together.
Since Covid appears to rapidly deplete Zinc as well as other nutrients like Vitamins C and D3, Dr. Vladimir Zelenco has apparently had success by combining HCQ, zinc and Azithromycin for out-patient use. He and others are now engaged in a retrospecive study of his treated patients and their outcomes compared with other Covid patients in his community who also suffered from Covid infection but were not treated using Dr. Z’s 3 part, 5 day treatment plan which costs $20. He treated older patients who had clear symptoms, and few were subsequently hospitalized and almost none died. I look forward to seeing their paper once it is published.
LikeLike
Here is a study done in Spain. HCQ does work. And Raoult is completely right. On what basis does remdesivir proof it works ??? Death rate is the same. This med is useless. If I contract the disease and I have to chose between HCQ and Remdesivir, I chose HCQ with my eyes closed. And then I add some Zinc into it. But HCQ is cheap. Remdesivir is an expensive drug from a big company sponsored by Fauci. That’s the difference here.
https://www.preprints.org/manuscript/202005.0057/v1
LikeLike
“It should be noted that while Raoult’s IHU hospital in Marseille boasts a very low COVID-19 mortality rate of 1.7% (while refusing to treat the very ill) it is still higher than the estimate for the rest of France which is 0.53% according to this study from Institut Pasteur. ”
Not a fan of Raoult at all but it is unfair to compare the mortality rate in his studies to the estimated infection fatality rate (0.53%) as the latter is necessarily much lower. As a reminder IFR = deaths / all infections (including the asymptomatics, undiagnosed etc.)
LikeLiked by 1 person
T, you mentioned the fatality rate in France is 0.53%? The European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea, as on April 22, 2020, reports for France 117 324 total cases, and 20 796 death cases. Expressed these stats (as you indicate) on % basis, gives a mortality rate for France as 17.73%.
LikeLike
See Salje et al (2020): Estimating the burden of SARS-CoV-2 in France
https://hal-pasteur.archives-ouvertes.fr/pasteur-02548181/document
just published a couple of days ago
LikeLike
You are attempting to compare the implied infection fatality rate of France to the case fatality rate of a hospital. That would be apples and oranges.
LikeLiked by 1 person
You mentioned above at ” Given the evidence that the coronavirus is apparently lethal for less than 1% of the infected……”. This cannot be correct!. In many countries, the mortality rate is >10%
LikeLike
This is lethality and not mortality, so learn first and talk later. Moreover, this depends on the amount of tests performed, so unreliable
LikeLike
Jhnny99, with respect, by definition lethality is the capacity to cause death, whereas mortality is the number of deaths from a particular cause. In the context of this discussion, I mentioned the mortality rate as the percentage of deaths within the population of people currently infected with COVID-19. Practically, every country in the world monitors a number of active cases and death associated with COVID-19, and these statistics are updated several times daily. These variables represent the cases reported by respective health authorities based on medical records and are independent of the number of tests performed.
LikeLiked by 1 person
To be able to comment you need to be aware of the difference between tested mortality and untested mortality. Most people who have COVID have not been tested.
LikeLike
Regarding the Mahevas study in Medrxiv.
Could the authors explain why 8 patients treated with hydroxychloroquine were counted in the control group?
Moreover, could they inform the public about the clinical outcome of these patients?
Is Raoult incapable of grasping the concept of “setting recruitment criteria and applying them consistently”?
Note that Mahevas et al are a French team of researchers. Raoult expects comity and collegiality from his French colleagues (and threatens them with discipline if they criticise him), but he does not extend the same courtesy.
Implying that Mahevas et al played fast-and-loose when assigning cases to groups (and complaining about lack of clarity in clinical outcomes) is especially rich and reaches Trumpian levels of hypocrisy. US rightwing politicians use this as a deliberate tactic. If your candidate has an obvious flaw – corruption or cowardice or multiple mistresses – you get in first and launch advertisements claiming accusing your opponent of immorality or cowardice or whatever. That way, if the other side tries to point out the flaw in your candidate, voters just roll their eyes.
Raoult is aping not only Trump’s language of “witchhunting” and “fake news”, but also his deployment of tactical hypocrisy.
LikeLiked by 1 person
Wrong. 100% wrong. I took it. It worked. You would too. Sorry, it works, I am living proof.
LikeLike
“You would fall for the same scam” is hardly a conclusive argument.
LikeLiked by 2 people
About Dr Barraud alias fluidloading (which never denied to be Dr Barraud), here is most of his attacks on Pr Raoult, look at this link
http://www.noelshack.com/2020-17-3-1587558555-r-barraud.png
Much more insulting than just “witchhunter”, which is a bit hard, but not insulting at all for me.
So, I understand the answer of the Marseille IHU .
LikeLike
Eh? You come to my site to complain that Dr Barraud doesn’t bring enough respect for Pr Raoult?
LikeLike
Thats a big fat lie… only in marseille France were people were treated with chloroquine the rate of deaths was the lowest in France almost 0, people didn’t die in marseille were Dr Raoult treated them, but in rest of France they did and in marseille there is also no more new infections, the same in Greece, they also use the protocol and are fine, this article is just nonsense, it’s harassment and because of those bad articles people were miss informed and didn’t get treated
LikeLike
excuse me in Greece we do not apply such protocol. Where did you hear that? This is not true. In any case, because of all this bruhaha (maybe this doctor partly to blame?) people were buying plaquenil in tons from the drugstore. Thank God they stopped him!
LikeLike
Look at the data please. Are you saying that Raoult is a fraud, Zelenko is a fraud, South Dakota is a fraud, the country of Bahrain is a fraud, along with 1000’s of doctors around the world? I understand being dismissive of one data source, but ignoring entire countries is highly unscientific.
https://docs.google.com/spreadsheets/d/1u7bETd3q9QVfO6y54jm_7Z5ZHTmoguUAetJHc2gwcj0/edit?usp=sharing
LikeLiked by 1 person
Zelenko is a fraud, but he seems to have shut up and left the scene when people started asking awkward questions about the current conditions of his clients and whether he was bothering to keep tabs on them.There were also legal issues about his rash decision to release a non-anonymised spreadsheet that identified his clients.
South Dakota? I don’t think there is any such place. Convince me that it exists!
LikeLiked by 1 person
Its amazing how trite and condescending a human can become. I guess even Clyde is some mothers precious child though.
LikeLike
Leonid! Noneya is being condescending!
LikeLike
I cannot agree more. Making huge profit out of this crisis by big pharma and their corrupted allies is the sole motive! Please stop manipulating people it doesn’t work anymore. In Morocco and South Korea the same protocol has proven extremely efficient with lowest mortality rates in the world. The treatment costs nothing and this is what is annoying them all!!!!
LikeLiked by 1 person
Raoult treats patients who come to IHU-Marseille, therefore statistically more motivated by symptoms than in the Pasteur survey.
Despite this, he had only 12 deaths out of 3039 patients, 0.4% is a succes that no one can deny.
And in the last study, he had 8 deaths out of 1061 patients, 0.75% is a bit more but it included 474 co-morbidities, you can’t tell that it’s only the easy cases.
There are many other errors in your paper, dear Leonid.
Unfortunately a (supposed) lie can’t be fought with another lie, but with the truth.
That’s why you failed.
P.S. : I agree that in Raoul’s treatment, HQ is probably a wrong way and AZ is perhap’s doing all the Job, but Raoult is not only HQ.
Seen from France he was a visionary that refuse this stupid general confinement and that very early asker fot the TTT’s way of the South Korea.
LikeLiked by 1 person
“Seen from France he was a visionary”??? You mean BFM TV let people think he was a visionary. Seen from France on April, 25, there does not seem to be an HQ miracle. Since you seem French, you understand every word of what is sung by the students in the students’ performance video. Can you deny this man is so hated that students who do not have a carrier yet are not afraid to go public on what it means to work in his institute? What kind of science performs an institute director who is insulted by his subordinates in a show and received a “coup de boule” (headbutt) by a coworker? Don’t tell me how a man behaves and what research he produces are two different things. I have almost 20 years of experience in academia to know that poor leadership produces poor work. With his communication method, Raoult has damaged how science is perceived. When the time comes to discuss research financing, what will the taxpayers remember of that story?
LikeLiked by 1 person
Pr Raoult is such a visionary that is predictions where false :
21/01/2020 : “Coronavirus in China: should we feel concerned?” “The world has gone crazy, 3 Chinese people die and it make a worldwide alert” ” (https://youtu.be/qoBoryHuZ6E)
17/02/2020 – “Coronavirus: fewer deaths than by scooter accident” (https://www.youtube.com/watch?v=00_vy-f22nE)
25/02/2020 – “Before we can influence mortality statistics in France, things will have to change a lot” in his “Coronavirus: a risk of pandemic?” video (https://www.youtube.com/watch?v=ZuE5CA6yB-Y)
I could also quote him on his “visions” about the climate but it’s out of his scope of proficiency
LikeLike
You have many valid points against Raoult methodologies, although the urgency of the situation excuses some of it.
However you don’t address the flawed Veterans study that Raoult criticizes, which is way worse than his studies on all points. You also write that Hydroxycloroquine doesnt work, there’s not a hint of evidence of that. You therefore have nothing scientifical in your approach as well.
LikeLiked by 2 people
I really don’t get this argument that “urgency of the situation excuses some of it”. I’d say that urgency implies reinforced attention, because a mistake could have enormous consequences when thousands of lives are on the line. OK we somehow face the unknown, but it’s not like we have no approach to deal with urgent situations, no knowledge gained from past pandemics and nobody except Raoult working on it. Politicians asking for an immediate solution to get people back to work asap in addition to damaged health systems in many countries, including the richest, already play a strongly negative role. If somebody has a hint that something might be working based on observation, then it should be presented that way. Scientists generally understand that and it is acceptable in urgent situations. But danger starts when you trick people. Nobody nowadays can ignore the role of media. Being approximate, not to say dishonest, and still go public in a situation like the present one is not like a quarrel in scientific journals that no one reads.
LikeLike
Untrue. This page is lying. Go read the paper that claims HCQ leads to higher death rate. Raoult is right. They gave all patients that were in the most critical state HCQ and then they conclude that HCQ increases deaths. Despicable manipulation. I stopped reading this page immediately because this is clearly a propaganda page.
Here is proof of a study one in Spain given HCQ early on. HCQ works. Period.
https://www.preprints.org/manuscript/202005.0057/v1
HCQ works like Tamiflu for the flu. You need to use Tamiflu withing 48 hours of your influenza infection or else it is useless. The same is true for HCQ. The side effects of HCQ are ridiculous. This medicin is approved for people with lupus and reuma. These patients take HCQ on a daily basis. Millions of people have been taking this drug for malaria in the past decades. If this drug would be really that toxic, it would never have been approved for those people.
LikeLike
Wow… from the moment you confuse cloroquine with hydroxycloroquine, everything you have written becomes invalid. just for starters. Costa Rica is using it using Wuhan methodology, you can check it out…what’s wrong with you, writing piles of shit? Ok, you don’t like the guy..you don’t like Trump…but it’s working, doctors have started using it and this pile of excrement you have written here will be forgoten and so will you!
LikeLiked by 1 person
Tell us more of this “Wuhan methodology”.
LikeLiked by 1 person
Wow ! You seem to be a great analyst. 12 deaths over 3000 people treated. 0,4% death rate. A full hospital of fake and lying medical staff ! That’s magic !
So continue your “better science” while they save people.
LikeLiked by 1 person
“He even treated 14 year old children with chloroquine as part of his 1000 patients trial (Table 1 here, recruitment age was >12 years old), which is actually quite illegal.”
It cannot be “quite illegal”. Either it’s illegal or it’s legal. Please either reference the law that was broken and explain how (which would be really valuable info), or delete that line.
LikeLike
It’s illegal : cf https://www.legifrance.gouv.fr/affichCodeArticle.do?cidTexte=LEGITEXT000006072665&idArticle=LEGIARTI000025457542
which is clearly the case here as it is an experimental treatment for this disease. Enrolling them if enough to violate the law even if they are part of the control group, since in a normal study groups are randomized and nor the doctors nor the patients know who is in which group. And in case you don’t know how patients are tested have a look at this ( https://health.ucdavis.edu/coronavirus/coronavirus-testing.html ), and tell me if you’d like to have your kids tested like this when it is NOT necessary they’d be part of the study. Once again minors cannot be included in a study unless they cannot be replaced by adults. This law has been made for this, to protect people and moreover children.
PS this French law the French transciption on EU law https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32014R0536
LikeLiked by 1 person
You misunderstand “study” and “clinical trial”.
He just healed patients that were showing up at his hospital, he wasn’t in a clinical trial and never was.
His study is merely a retrospect study and the control group he used is just people who refused or couldn’t receive the treatments for various reasons.
Childs are going to be tested as well in a case of a pandemic, remember, we have to heal the people.
the “Oh no, don’t test my child with PCR, let him die of unknown reason” is not what a decent parent is going to say.
We do have laws in France, and they respected it. The ones that are border-line are the one insulting a peer on a emotional basis, even sending death threats to him.
We can see all those greedy for popularity wanna be expert doctors with over 10+ years in their field and nowhere on the level of Raoult showing up in ALL medias on a daily basis, criticizing his work.
And what now? It’s quite clear that he was right, he’s having the lowest case fatality rate in the world at his hospital/IHU and people are still dyeing at alarming rates elesewere, while still insulting his work because it was not “randomized”.
I quoted a bit of the french parlement investigation on coronavirus crisis handling in France and Raoult answered some question, the very last one (question):
“the question I ask myself and I’m not the only one to ask it (start doubting tone like he already knows the answer),
but why, oh why, you didn’t make clinical trial worthy of its name from the start, that could answer permanently Yes or No, the HCQ has effects, why did you keep in your niche paper … I know all your studies on Rickettsies, I know all your studies on maxivirus etc so I know your science well established, you knew very well that by publishing those “pseudo” trial, “pseudo clinical trial”, there were not acceptable by anyone, when we end up on a publication with 6 patients (he had 23, perhaps 6 in one group), we know very well that this i not a clinical trial, so why did you not do this clinical trial, it all bothers us” … You can see where it’s going”
The answer, I’ll let you translate it yourself though google, this is the word for word answer of Raoult on why he didn’t do a “clinical trial worthy of its name”: (added words to ease translation in parenthesis)
Non, je, je, je suis pas d’accord avec ça, euh, d’une part ce que nous avons fait, c’est ce que, ce que, ce qu’il se fait de plus simplement, c’est à dire quand on fait un essai thérapeutique si vous voulez, quand les choses deviennent significative, on, on a, c’est, c’est de l’éthique basal hein, l’éthique n’a rien avoir avec la méthodologie, c’est deux choses distincte, l’éthique basal c’est que quand on a la preuve que quelque chose marche, et on doit le faire à mi-chemin, quand on a la preuve que quelque chose marche on arrête l’essai et donc je suis désolé que vous n’aimiez pas mon essai, moi je l’aime beaucoup et je trouve qu’il a toute les bases d’un essai de la seule manière de faire des essais qui est de faire des essais comparatifs et d’avoir une différence significative et contrairement à ce que vous dites et ça alors là, je m’excuse mais c’est une erreur RADICALE, moins il y a de gens quand c’est significatif alors plus c’est significatif. Si vous êtes obligés d’avoir dix mille personnes dans un essai pour montrer une significativité c’est qu’il n’y a aucune différences, parce que je vais vous dire, il y a quinze pour-cent des gens qui ne prennent même pas les médicaments que l’on leur prescrit, quand vous cherchez une différence de 1%, vous n’êtes plus dans de la médecine, vous êtes dans du fantasme méthodologique donc tout essai qui comporte plus de mille personnes est un essai qui cherche à démontrer quelque chose qui n’existe pas et je suis désolé mais c’est une des bases de la statistique et je vous assure que je suis un très bon méthodologiste, donc c’est du fantasme qu’on vous répète… qu’on répète à tour de bras qui est véhiculée par des gens qui sont des méthodologistes qui ne comprennent rien à la science. La méthodologie n’est pas de la science, c’est un outil de la science, cela n’a rien avoir (ce n’est pas la même chose). Donc il faut pas me dire que les essais ne sont pas (des essais) … parce que vous avez dit avant et c’est vrai, je suis un grand scientifique, je sais ce qu’est un essai et je peux vous dire il y a des dizaines de traitement que j’ai inventés qui sont dans tous les livres de référence médicaux et celui là y sera aussi, je vous le dit, nous verrons. Mais je peux vous dire et il faut arrêter, il faut regarder les livres médicaux, il faut regarder en maladies infectieuses combien il y a d’essais… combien il y a de thérapeutique qui sont utilisés actuellement qui ont été basées sur des essais randomisés et vous verrez, il y en a pas beaucoup et le peu qu’il y a étés en particulier pour le Sida et étaient totalement inutile parce qu’il suffisait de faire des charges virales.
Donc, c’est pas vrai, c’est de l’intox, c’est pas vrai et ça disparaîtra comme c’est apparu il y a une vingtaine d’année, c’est de l’intox, je vous suggère d’ailleurs plutôt que… vous avez qu’à le lire car c’est intelligent, sur la version de wikipedia en anglais, vous avez qu’à lire, vous verrez qu’il y a la moité qui dit “voilà il faut faire des essais randomisés” et l’autre moitié qui dit “voilà pourquoi il ne faut pas en faire” et vous verrez que je ne suis pas isolé dans ce monde et que d’ailleurs tous les gens qui ont critiqués ça, je le redit, d’ailleurs et il faut le lire et il faut écouter ce que je dit, tous les gens qui ont critiqué ça n’ont publié que des essais comparatifs non randomisés, il n’y a pas un essai français randomisé comparatif, il n’y a pas même un essai français qui ait le degrée d’isolement des stratégies thérapeutique comme le notre, zéro.
C’est que des gens qui dans les hôpitaux ont traités un peu comme ils voulaient qui a la fin on dit “regardez comment on compare”, donc il faut pas mettre les choses à l’envers, j’étais avant un grand scientifique et je suis resté un grand scientifique après avoir publié ça.
Everywhere you see “essai” translated as “test”, it’s more a “clinical trial”.
LikeLike
source: https://youtu.be/K71LcQDnlOg?t=10937
LikeLike
If you download the original Renesto et al. blot and examine it with Fotoforensics or just Photoshop, it is easy to see that all of the bands/lanes are pasted in. It is a complete collage. This guy has been trolling science for years.
LikeLike
Dear Owlbert, please share your visual analysis!
LikeLike
Put the PNG version through level sweep analysis, and it shows blocky halos around pasted-in elements, including text, bands and lanes. I can’t insert graphics here.
LikeLike
Upload to imgur.com and add link, as Zebedee always does!
LikeLike
Independent Science Journalist and Cartoonist. The author is a cartoonist. Why don’t you talk to doctors that are really using HCQ in the hospital and ask them if it works? Its clearly to early to use data and studies. We as doctors need to think about how things work and why they work. We need to prevent the Cytokine storm. Treating after the storm is too late. The day you get the disease and the day you get treated really matters. If you treat shingles after 48 hours Valcyclovir is not effective. If you treat Infulenza with Tamiflu after 48 hours Tamiflu is not effective. If you put oil in your motor after you drive really matters. Its all the same. Timing is everything. Well almost everything. My point is the timing of treatment is really big deal. Pubmed as data on the Chinese invitro study of chloroquine.
LikeLike
Your article is obviously not written in an objective manner. You undermine your credibility with your extreme polemic personal attacks. Have you read Dr. Magagnoli et al’s study on outcomes of hydroxychloroquine for COVID-19 patients in the VA and checked whether Dr. Raoult’s criticisms of it are valid? I have and conclude Dr. Raoult’s rightly points out its serious flaws.
LikeLike
Oooh, that’s rich. I think it’s better to focus on the serious flaws of Rauolt’s ‘studies.’ And if we want to talk about undermining credibility with extreme polemic personal attacks, we should look at what Raoult is doing and has done for years against detractors.
LikeLike
Pingback: De linke weekendbijlage (17-2020) - Kloptdatwel?
The dismissal of hydroxychloroquine with zinc, etc. treatments used early at the onset of covid-19 by the mainstream media and medical elites like yourself is a poster child example of the battle between integrity vs ideological rigidity. The blame for thousands, if not millions, of covid-19 deaths will soon become abundantly clear being laid upon these two groups of ideoligists referenced above. That is if the truth is allowed to prevail.
LikeLike
Very serious,very,very serious .Stay “independent Cartoonist ” . Will be better for all of us dear Mr.Nobody.
LikeLike
At the moment we don’t have any treatment that is efficient for covid-19. This is not a surprise, based on experience from SARS-Cov, MERS-Cov and seasonal influenza virus.
History has learned us that vaccine is the only efficient treatment.
Please forget politics, stupid conspiratory theories and ideology and take care while waiting for a vaccine to be developed.
LikeLiked by 2 people
I totally agree with Morty!
LikeLike
Pingback: Figure di palta e piedi d'argilla - Ocasapiens - Blog - Repubblica.it
Pingback: Hydroxychloroquine and the price of abandoning of science- and evidence-based medicine – Science-Based Medicine