The German trachea transplanters Heike and Thorsten Walles fitted three patients with pig-intestine-based airway grafts. They responded to my inquisitive reporting about these with a court injunction, the trial takes place this week, on March 16th. A commission of their Unversity of Würzburg initially absolved Walles of all suspicions of research misconduct, only to start the investigation anew as evidence of heavy data manipulation in their papers emerged (see my previous report). Roland Jahns, specially recruited as medical expert from the same University Clinic Würzburg where both Walleses work, was dismissed after he insulted me as “pseudoscientist” to defend his colleagues’ questionable attitude to data integrity, medical ethics and patient welfare. A new expert will be recruited, but Jahns did reveal some clues to what happened to the two last Walles patients operated in Stuttgart in 2007 and 2009, just before they received their professorships in Würzburg.
It appears Thorsten Walles issued two radically opposing versions of the 2007 patient’s state. In his publications, he presented the intervention as “compassionate use” case and the patient as stable, but in need of innovative strategies to cure his condition. In the medical file however, Walles described the patient as terminally ill and dying from cancer. The intervention to replace his airways with a never-before-tested pig-intestine large patch was presented as a palliative approach, which however turns the entire concept of either palliative care or compassionate use care on its head. In any case, the graft had to be removed after only 2 weeks, the patient died four weeks later due to massive bleeding and multi-organ failure. Walles decided that this disastrous incident had nothing to do with the transplant, so when they recruited their next patient to sign an informed consent in 2009, they simply didn’t tell him what happened to his predecessor. That last patient was also post-suicidal and in psychiatric treatment (though not yet officially of unsound mind, his mental state further deteriorated later on).
No ethics votes, no animal experiments, no truth
Importantly, no ethics vote was obtained, for neither of the transplants. The fact that the Ethics Commission of the University Tübingen declared itself as not responsible for compassionate use cases, was presented in publications and in official announcements as proof that a valid ethics vote was granted. And as I already reported before, there never were any animal experiments. Did the patient know this? Walles used to and even now do spread false claims about the alleged animal testing of their tracheal grafts, which were in reality never performed (see here). Thus, one has no reason not to assume these two professors misinformed all their patients as well. Would these people have signed their “informed consent” to the untested transplants if they knew they were indeed the Guinea pigs? All three are dead now, and the Würzburg court will now decide whether to follow Walles’ demand that the public has no right at all to stick its nose into how and why they died.

This is what the Würzburg Commission originally passed as their final decision on February 20th, before my appeal on March 6th led to a total reset of the investigation:
“The patients were thoroughly informed about all procedure-related risks both in written and in oral form and gave their informed consent. Prior animal testing is not required when aiming to treat a patient individually with a new type of therapy or a new type of medicinal product under the frame conditions of compassionate use. Additionally, in all the three cases it would have been too late to carry out such tests.”
We will see below how thoroughly informed the Stuttgart patients were. And as to why animal testing was deemed unnecessary: because an earlier operation in Hannover, which Walles performed in 2003 together with Paolo Macchiarini, was presented as a resounding success (Macchiarini et al 2004 and Walles et al, 2004),despite harsh criticism from peers (Grillo, 2005). However, that patient died 16 months later, quite possibly of his recurrent cancer, yet no one analysed how his tiny cent-coin-sized transplant patch fared by that time (see my report here, patient 1). A follow-up paper by Walles and co-authored by Macchiarini (Walles et al 2005) presented also only a 12-weeks follow-up. It reads that the patch was overgrown by a kind of fibrous scar tissue, the defect it was supposed to cure did not disappear, but was said to become smaller (from 12 x 9 mm to 9 x5 mm). The authors concluded:
“In the light of previous unexpected (sometimes fatal) clinical experiences with bioartificial grafts (5 [Simon et al 2003, -LS]) further studies are needed to address questions regarding the healing behavior and mechanisms of bioartifical implants.”
“Further studies are needed”
In 2004, both Walleses left Hannover and moved to Stuttgart, where Heike Walles continued to develop her pig-intestine technology at the Fraunhofer Institute for Interfacial Engineering and Biotechnology (Fraunhofer IGB). Animal experiments were deemed unnecessary, both by Walles and Fraunhofer IGB, which is a federally-funded materials engineering research institute keen to dabble in medicine, despite having apparently very little clue of biomedicine or biomedical ethics. But with enough funding, confidence into your own talents grows exponentially. In 2007, the studies announced in the 2005 paper began, on other human beings, followed by one fatal clinical experience, and one suicide of a clinically mentally ill patient. Were those really entirely unexpected?
For some reason, Walles did not do a good job describing the preoperative state of their patient from 2007 (patient 2 in this report of mine) in the two publications describing him (Walles et al 2008, Mertsching et al 2009). Remarkably, none of these two papers tells anything about the graft transplantation into his airway and what happened after. Also omitted was the minor fact that the patient died following the operation to implant his airway graft, long before either of the two papers was published. One paper (Walles et al 2008) described the use of the lung ventilation machine when this 63-year old patient was receiving his airway graft, to close “a 6 x 2–cm defect of the anterior esophageal wall extending into the posterior wall of the remaining trachea”:
“A 63-year-old man was admitted for defect closure of an extensive esophagotracheal defect that had developed following laryngectomy and suprajugular tracheostomy by a bioartificial vascularized esophagotracheal patch.4”
The reference 4 linked to Macchiarini et al 2004, by which this meanwhile deceased 63-year old Stuttgart patient suddenly turned into his predecessor from Hannover, who died in 2004, aged 59. The patient’s pre-operative state description also overlaps with what Walles declared under oath to court when issuing injunction against me. No end-stage cancer or any terminal condition was mentioned there either. Jahns, the sacked Würzburg Commission expert , declared however that this description was not correct. According to Jahns’ studies of medical files, this patient was suffering from terminal end-stage cancer, the operation was seen as palliative, to improve the quality of his last days. This however would go against the entire concept of compassionate use (in German Individueller Heilversuch), since a cure of the patient’s actual disease (cancer) was neither possible nor even proposed here. A dying cancer patient was basically invited to participate in a medical experiment to test a novel tracheal transplant, which even if successful would have done nothing at all to extend his life. Could it at least have been of any use to reduce the patient’s suffering in his remaining last days? There was nothing at all to suggest this, aside of the educated guess of the Walleses. But plenty of risks, in fact an entire Pandora ’s Box full of them.
Large-animal experiment?
It seems therefore, a human gave his agreement, where a pig or a sheep would have been a more appropriate, but paperwork-wise much more cumbersome, candidate. Research as main rationale for a medical intervention on a patient however is explicitly not allowed by law to justify compassionate use in Germany. This patient however was presented to the Ethics Commission of the medical faculty of the University of Tübingen as a compassionate use case. The Commission declined to issue a vote, because, as its head Dieter Luft explained to me:
“The Ethics Commission is only responsible for the advice on scientific research studies, not however for the advice – or even approval- of single compassionate use cases. Which special requirements are placed on the clinician, this you can learn from the decision of the Federal High Court (VI ZR 55/05, position BGH Z 172,1).”
These court-imposed requirements deal primarily with informed consent, and I will come to that below. How Walles described his patient to the Ethics Commission: this information is secret. Peculiarly, Jahns declared that it did not matter a bit if Walles misrepresented the patient’s preoperative state in his publications or elsewhere, but what mattered only was what his colleague wrote into the (confidential) patient’s medical files. Fortunately, with Jahn’s sacking this logic will be hopefully also gone from the Commission’s re-opened investigation. Of course it is also possible that Walles did not write untruth in his papers but put false information into this patient’s medical files instead. I am not sure if it makes the situation any better. The compassionate use of the pig-intestine airway graft ended in a disaster for the patient either way.
Bled to death
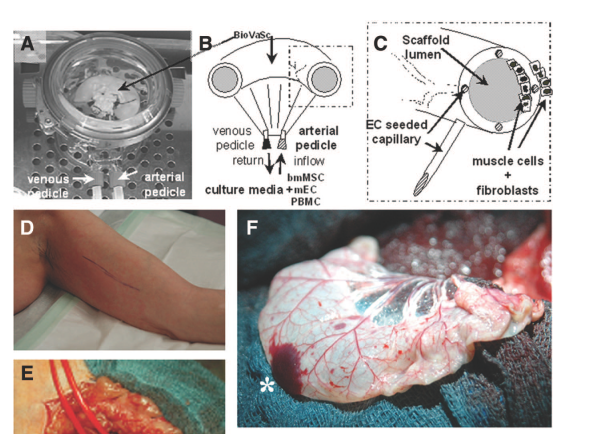
In the other article featuring that 2007 patient, Mertsching et al 2009, a test of this pig-intestine-based graft in his upper arm was described (which Walles followed the next week with an airway transplant). That paper doesn’t address the preoperative medical state of the patient at all, but describes this noteworthy incident caused by blood-diluting treatment (highlights mine):
“The aggressive anticoagulation protocol resulted in hematoma formation at the operation site necessitating removal on the second postoperative day. Here, several capillaries at both margins of the BioVaSc were identified as the sole source of bleeding. The bleed was staunched by electrocautery. At explantation after 1 week, the bioengineered tissue was viable, and the embedded vascular network was patent. On bioartificial tissue explantation, we detected a hematoma surrounding the bioartificial transplant, but no active bleeding”.
Now, this is what the patient died from, according to Jahns:
“The transplant integrated only poorly due to a pre-existing severe arteriosclerosis of the patient and necrotized in spite of the blood thinning attempts (to improve circulation) and was removed on day 14 after implantation (24.07.2007); The patient died only four weeks later after mass bleeding (27.08), bilateral inflammation of the lungs due to aspirated blood (29.08) on 31.08.2007 at the intensive care unit in multi-organ failure”.
The patient was given anti-coagulants despite a bad experience with them regarding the transplant less than two weeks ago. As a cardiovascular specialist explained to me, a multi-organ failure in such a situation can be caused either by an internal haemorrhage or sepsis (blood positioning). According to Jahns, the patient was about to die anyway:
“The necrosis of the transplant was not the cause of death, but only the consequences of the mass bleeding 4 weeks after graft removal!”
Misinformed consent
Less than two years after this patient suffered multi-organ failure and bled to death in the aftermath of the tracheal graft operation, Walles recruited in April 2009 Pavninder Singh (patient 3 in my earlier report), a victim of attempted suicide who burned his oesophagus and airways by intentionally swallowing oven cleaner liquid. According to Jahns, this patient was diagnosed with “stress reaction” or shock and treated psychiatrically (though described as “stable”). As before, no ethics vote was obtained, as it was once again seen as compassionate use case. The patient was invited to give his informed consent, yet nobody ever told him what happened to his predecessor. Jahns has confirmed this to me; he also saw no need to disclose this death to the patient Singh and the public. The original patient information sheet and the consent form which Singh signed are not being released either, neither by the Clinic Schillerhöhe nor by the University of Würzburg, despite the fact that the patient expressly waived all confidentiality (i.e., when he was still alive). A copy of his medical file was in fact handed out to the journalist Bernhard Albrecht, who then wrote the revealing book about that operation. On the other hand, I am denied even the most basic insights. But even from what I already learned: whatever Singh signed to Walles, it was sure not an informed consent, but a grossly misinformed one.

Another question is if he was actually in the right state of mind to agree to experimental procedure which then threatened his life with the ensuing heavy, half-a year-long inflammation in his throat. We also know that this transplant most likely contained unacceptable levels of endotoxins, inflammation-causing bacterial residues from the pig intestine (see my earlier report). Noone bothered to measure endotoxin content until around 2010-2011, when 3 patients were already operated with the tracheal grafts. Then suddenly, values of up to 560x above the allowed limit of 0.25 EU/ml were detected. In any case, the immunogenic response to the pig-intestine-grafts was never tested in animals, never mind any tests of their performance inside airways.
Jahns denied the endotoxin danger during the March 6th meeting in Würzburg or that the inflammation was related to transplant. I asked him then if Singh received that (likely endotoxin-contaminated) pig-intestine graft while the inflammation was already raging. Jahns denied this also, but once again, Walles’ own publication Steinke et al 2015 claims something different and suggests that an already present severe inflammation was made even worse (highlights mine):
“Owing to his complex tracheoesophageal injury, the ongoing severe intrathoracic inflammatory reaction, the very limited treatment options, and the reproducible good results in previous tissue-engineered airway transplants, it was decided to offer the transplantation of an autologous bioartificial repair tissue for airway reconstruction.7,8”
Which “reproducible good results”? The obviously useless, scar tissue-overgrown tiny patch from 2003 inside the late Hannover patient (linked as reference 7, Macchiarini et al 2004), or Singh’s direct predecessor who bled to death in 2007 after his transplant was removed (reference 8, Mertsching et al 2009)? I do agree with “reproducible” here, but “good”?
After the operation, Singh’s tracheostoma was closed by Walles because he decreed that his transplant cured the airway defect. It most obviously did not, other doctors had to re-open the tracheostoma. Jahns however declared:
„the tracheostoma was necessary due to scar tissue formation in the larynx area, it stood in NO connection with the transplant!
Singh mentally suffered after the operation and the reopened tracheostoma, he became clinically psychotic and was treated in the psychiatric hospital. In late 2011, he undertook another suicide attempt, where he sadly succeeded when he placed himself on the rails in front of an approaching train.
Why?
The medical indication of the Walles’ tracheal transplant was unclear in Singh’s case as well. The main damage caused by the oven cleaner was on Singh’s oesophagus and epiglottis, the tracheal defect was apparently rather stably taken care of by the tracheostoma and probably the least urgent of his chemical-burn induced malaises. Jahns did declare to me during our conversation on March 6th that the transplant was necessary to cover a large fistula, a hole between his oesophagus and trachea. However I pointed out to him that according to the publication Steinke et al 2015 the fistula was apparently dealt with in a traditional way, with a standard suture:
“The tracheoesophageal fistula was then opened and the esophageal defect was closed with an interrupted resorbable suture (Vicryl 4.0; Ethicon, Norderstedt, Germany)”.
We didn’t not speak of fistula afterwards. In his later email, Jahns assured that Singh’s transplant was never removed, though it is not clear if he had access to other medical files, namely those not written by Walles. The latter stayed away from Singh for over two years, except of one biopsy performed somewhere in 2011 (exact date and even part of the year apparently secret, see this report). Other clinicians rescued Singh from inflammation, re-opened his tracheostomy and reconstituted his oesophagus, while his absent surgeon Thorsten Walles and the transplant-maker Heike Walles went on to celebrate themselves in all the media.
Singh’s post-operative complications or his death were utterly unmentioned in Steinke et al 2015, quite the opposite. Originally, the Würzburg commission decreed (highlight mine):
“The Commission cannot follow the allegation that the failure of the procedures had been obscured in publications. In particular, this applies to the article Steinke et al., which refers to a biopsy conducted two years after the operation. Although the article was only published at a time when the patient had already died and does not mention this fact explicitly, the Commission is convinced that the patient’s death was not related to the procedure in any way. The time and place of the procedure can be derived from a reference to a preceding article about the operation. Expressly stating this again in the subsequent study would have been possible but, due to the limited epistemological interest of the paper, was not mandatory”.
When I spoke in front of the Würzburg Commission on March 6th, its members admitted that such a “preceding article” does not exist. Singh only featured in that one Walles paper, namely Steinke et al 2015. This somewhat fits to the other assertion of the sacked Commission member Jahns, namely that asking a wrong institution for an ethics vote (possibly by misrepresenting the patient’s true state) is equivalent to the actual obtaining of an ethics vote.
It does not look at all that any of the three tracheal transplant operations was a success of compassionate use care; in fact serious suspicions manifest that these interventions were unethical or actually even illegal. The federal authority in the position to judge this, the Paul-Ehrlich-Institute, keeps breaking a federal law by refusing to release any information. Walles sure nicely padded their publication records, by making a total of 6 research papers from those dead patients whom they misinformed, together with the scientific community and the public. In the Walles’ written works, both Singh and the patient from 2007 are alive and well, even in papers which appeared long after these patients’ death. The journal Tissue Engineering Part A, where Steinke et al 2015 was published, also prefers this happy-end version to the reality, as they made unmistakably clear.
Update 25.03.2017. I received a letter from the Ethics Commission in Tübingen, following their meeting from March 13th to discuss Walles transplants. Full letter is here:
“As you write correctly in your most recent article [this one here, -LS], the Ethics Commission at no time issued a vote on the compassionate use cases of Prof Dr. Walles, due to its lack of competence for compassionate use cases.
The compassionate lies is in the sole responsibility of the treating doctor, who, as you write in your article, must adhere to the special demands of the Federal Court regarding the informed consent. Also here the Ethics Commission lacks a reviewing competence, in accordance to the legal provisions of the state Baden-Württemberg.
The formulation of the investigative report by the Commission the University of Würzburg is, as far as it refers to our Commission, probably misleading”.
If you would like to support my court litigation financially, donation amount doesn’t matter, please go to my Patreon site or contact me.
Donate!
If you are interested to support my work, you can leave here a small tip of $5. Or several of small tips, just increase the amount as you like (2x=€10; 5x=€25). Your generous patronage of my journalism will be most appreciated!
€5.00


Recent article includes ghastly details of failed cadaveric trachea transplant performed in 2010 by Macchiarini in Russia: http://www.cesurg.ru/en/jarticles_cesurg/111.html?SSr=500133a20015ffffffff27c__07e00a180f322a-7c85
LikeLike
Pingback: No animal testing before Walles tracheal transplants, admits Fraunhofer Society – For Better Science
Good luck tomorrow, I hope it turns out well for you.
LikeLike
Check this out! Two articles of Wuerzburg University which say that animal experiments were successfully done:
http://www.ccc.uni-wuerzburg.de/ueber/sonstige_einrichtungen/comprehensive_cancer_center_mainfranken/aktuelles/single/artikel/wuerzburge-5/
https://www.uni-wuerzburg.de/sonstiges/meldungen/einblick_vorschau/single/artikel/lesung-pi/
LikeLike
“Oh what a tangled web we weave, When first we practise to deceive!”
The lies are so broad and deep that they can’t find them all.
LikeLike
Cool! The two articles have been removed (are they reading this blog?). Chronically sloppy reporters?
LikeLike
It’s possible to find them in the wayback machine (internet archive) and one of them through google cache. I have copies if anyone wants them.
LikeLike
I offer the backups in the update at the end of this article: https://forbetterscience.com/2017/01/23/no-animal-testing-before-walles-tracheal-transplants-admits-fraunhofer-society/
Since the state of Bavaria has no FOI law, anything the University of Würzburg now removes from internet is gone for good, no inquiry will ever be able to recover the removed documents.
LikeLike
Pingback: Boletim de Notícias, 16/mar: pesquisador aponta negligência com febre amarela | Direto da Ciência
Pingback: Würzburg misconduct Commission acquits Walles, dismisses biased medical expert, restarts anew as data manipulations flood in – For Better Science
It’s possible to find them in the wayback machine (internet archive) and one of them through google cache. I have copies if anyone wants them.
LikeLike
Pingback: Retraction, and another looming misconduct finding for Macchiarini and Jungebluth – For Better Science
Pingback: Evidence is a lie, listen to our authority, say Walles to scientists – For Better Science
Pingback: Will words or actual evidence count in the Walles case? – For Better Science
Pingback: Ciaran’s success story – For Better Science
Pingback: Walles misconduct investigation in Würzburg widens inside a federal cover-up; Jungebluth’s dissertation whitewashed in Hannover – For Better Science
Pingback: Paul-Ehrlich Institute admits to have approved Walles tracheal transplant over phone, without questions – For Better Science
Pingback: Walles court trial against me ends with “amicable settlement” – For Better Science
Pingback: “Me llamo Paloma Cabeza Jiménez”: Macchiarini victim speaks out – For Better Science
Pingback: Megagrant, the Russian docu-novel of Paolo Macchiarini – For Better Science
Pingback: Hannover Medical School MHH: where doctor careers matter more than patient lives? – For Better Science
Pingback: New government cash for trachea transplanters Videregen – For Better Science
Pingback: The Lancet, UNSW and Khachigian's cancer cure – For Better Science
Pingback: Tiwari’s IAAM honours Magdeburg – For Better Science